Anatomy
Anatomy
The basic anatomy of the female vulva consists of the mons pubis, the labia majora, and the labia minora. The clitoris superiorly is located under a hood or prepuce that splits to join the labia minora on either side of the introitus. (Fig. 81-1). Beneath the apex of the frenulum the urethral meatus can be found. The labia minora converge posteriorly beyond the vaginal opening to form the posterior fourchette, or remain separated as they attach to the perineum.
The labia minora themselves lack hair follicles and subcutaneous fat, unlike the labia majora. Measurements of the length of the minora range from 2 to 10 cm.11,12 Due to wide anatomical variation of labia minora size and shape, it is difficult to define true labial hypertrophy. In a review of 163 labiaplasties, Rouzier et al. designated labial hypertrophy if the distance from the base to the edge is greater than 4 cm.13 Most women who request labiaplasty dislike the protrusion of the labia minora beyond the labia majora in the standing position.14 Since minora protrusion is dependent upon labial length, shape, and coverage by the labia majora, measurement of labial length alone is not a useful parameter in planning labiaplasty.
The blood supply to the vulva is derived primarily from the external and internal pudendal systems, as well as smaller contributions anteriorly from the obturator and funicular arteries. In 2015, Georgiou et al. defined the arterial supply of the labia minora in 10 cadaveric specimens using contrast CT and rotational angiography.15 They described the central artery extending from the base of the labia to the tip to be the dominant arterial supply to the labia minora. This artery located just deep to the mucosa is supplied primarily by the internal pudendal system posteriorly. A small anterior
branch from the external pudendal system was present as the secondary feeder to the central artery (Fig. 81-2).
The nerve supply to the vulva consists of the genital branch of the genitofemoral nerve, the ilioinguinal nerve, the pudendal branch of the posterior femoral cutaneous nerve and the inferior hemorrhoidal nerve (Fig. 81-3). The dorsal nerve of the clitoris is analogous to the dorsal nerve of the penis and is a terminal branch of the pudendal nerve. It courses along the ischiopubic ramus and anteriorly pierces the perineal membrane to supply the clitoris. Due to its deep location, injury to this nerve is unlikely during labial surgery. Superficially, genital corpuscles are rapidly adapting mechanoreceptors present in the labia minora, clitoral hood, clitoris, and the vaginal vestibule. These microscopic coils of nerves are highly sensitive to touch and vibration.
Controversy exists regarding the potential reduction of labial and or clitoral sensation after labiaplasty. Despite the documented high satisfaction rate postoperatively in both sexual satisfaction and emotional well-being,16 doubts exist regarding the potential for nerve injury or decreased sensation. Recently, this theory has been refuted. A recent cadaveric study demonstrated that the nerve density of the labia minora is heterogeneous.17 Additionally, Placik et al. showed that sensation to light touch was maintained and actually improved after labiaplasty and clitoral hood reduction.18 Surgical procedures to alter the vulva can therefore safely be performed by trained surgeons familiar with the anatomy.
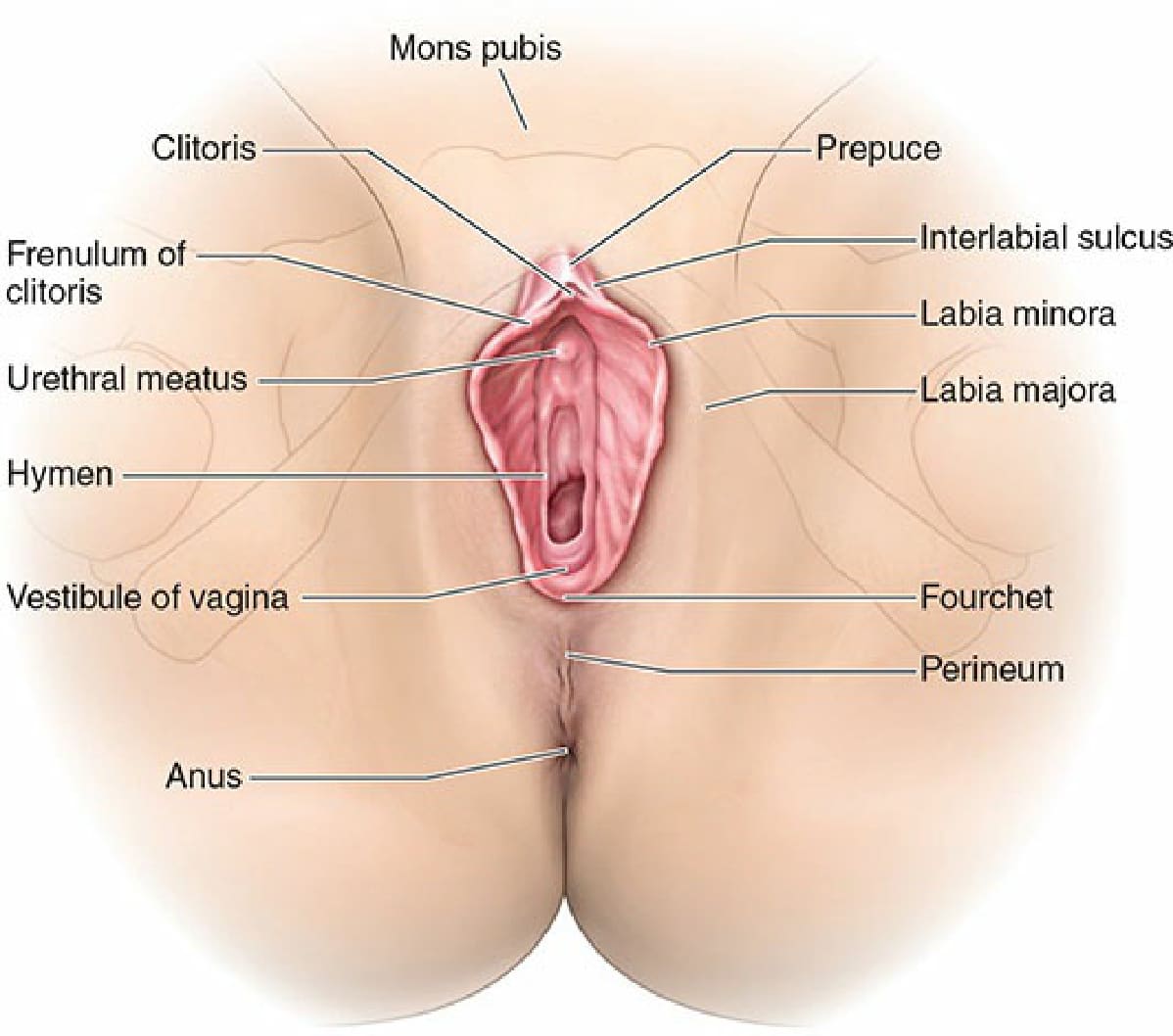
Figure 81-1. Anatomy of the external female genitalia.
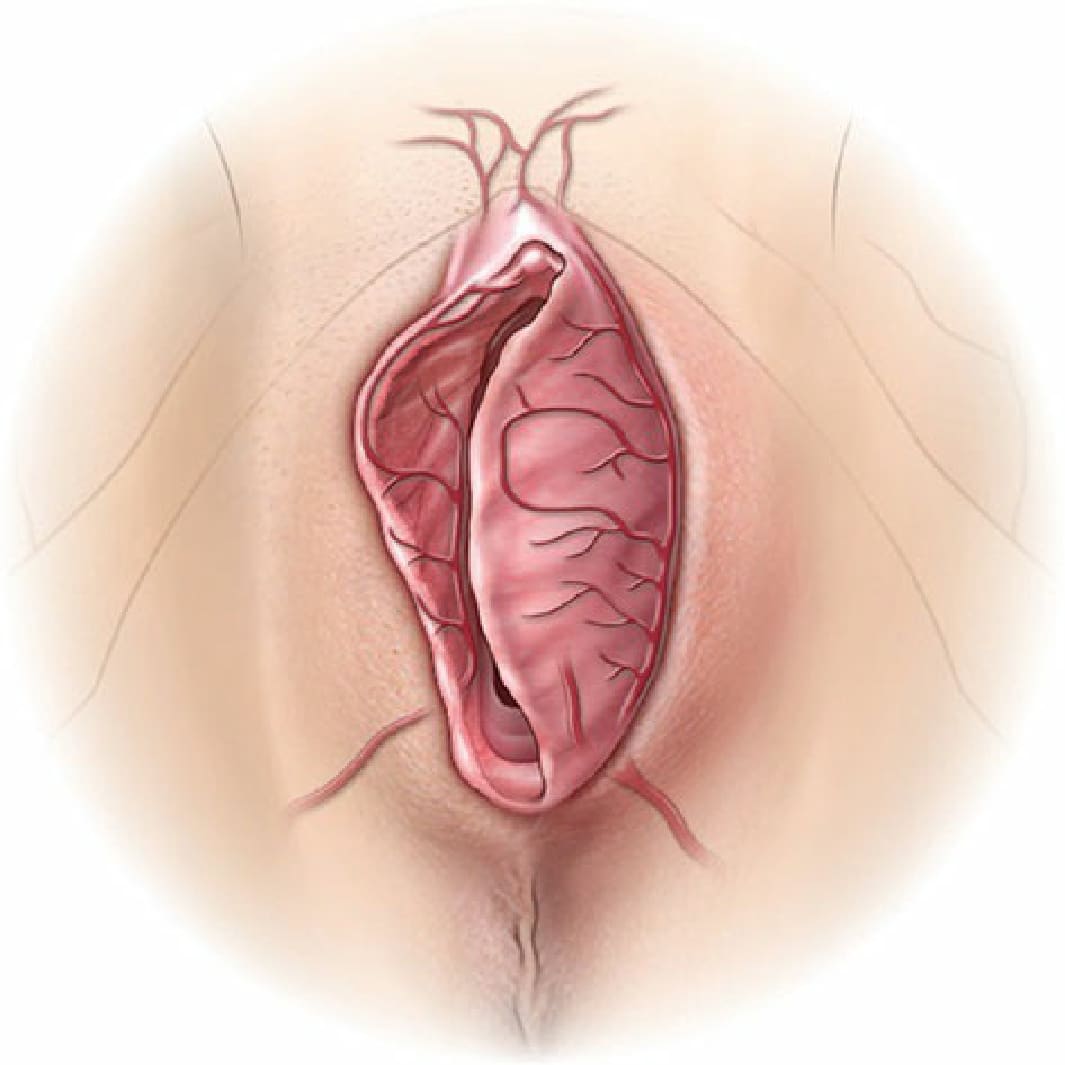
Figure 81-2. The blood supply to the vulva is derived primarily from the external and internal pudendal systems, as well as smaller contributions anteriorly from the obturator and funicular arteries.
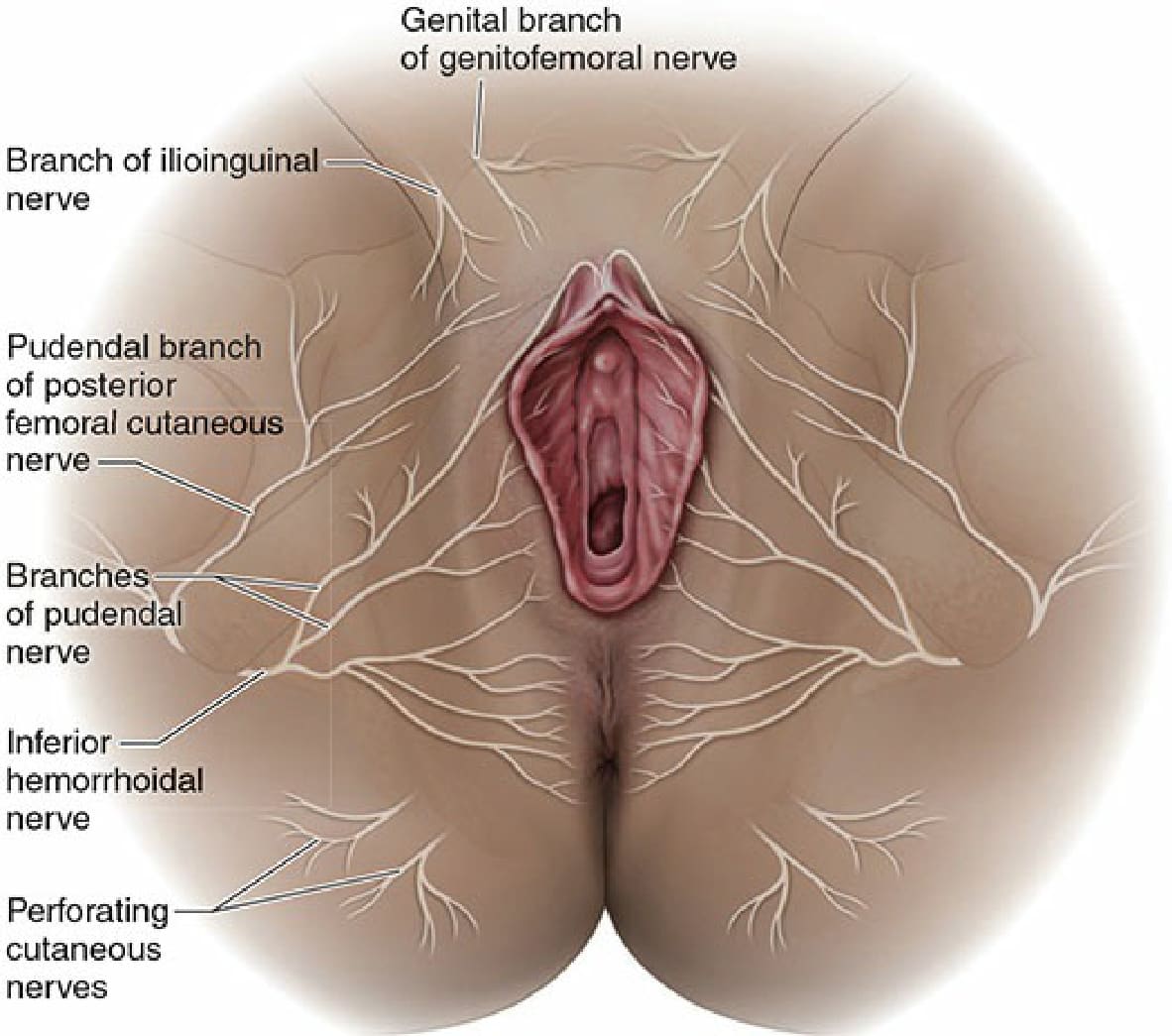
Figure 81-3. The nerve supply to the vulva consists of the genital branch of the genitofemoral nerve, the ilioinguinal nerve, the pudendal branch of the posterior femoral cutaneous nerve and the inferior hemorrhoidal nerve.