LIGHT-BASED THERAPIES
LIGHT-BASED THERAPIES
Various light, laser, and energy devices have been used for hand rejuvenation. These include IPL, photodynamic therapy (PDT), Q-switched (QS) lasers, 1,320-nm neodymium-doped yttrium aluminum garnet (Nd:YAG) laser, fractioned 1,550-nm erbium-doped laser, fractioned 1,927-nm thulium laser, 2940-nm erbium-doped YAG (Er:YAG) laser, and fractioned 10,600-nm CO2 laser (Table 80-3). Since the dorsal hand skin is thinner, has a decreased vascularity, and fewer pilosebaceous units than the face, the fluence, density, and number of passes should generally be reduced to minimize recovery time.21
A frequent patient complaint about their hands is the development of solar lentigines and macular seborrheic keratoses. These rarely resolve permanently with topical superficial peeling agents. Selective photothermolysis of the pigment within melanosomes, such as that employed by QS lasers, is highly effective.55 Melanin has a broad spectrum of wavelength absorption across the optical spectrum. Preferred lasers have wavelengths from approximately 500 to 755 nm. Since the thermal relaxation time
of melanosomes is only 0.25 µs, short pulse durations are optimal.51 For this reason, the QS ruby laser (694 nm), QS or picosecond alexandrite laser (755 nm), and the frequency-doubled QS or picosecond Nd:YAG laser (532 nm) are most often employed (Table 80-4).56,57 These devices deliver pulse durations in the nanosecond and picosecond range, respectively. Usually a one-time treatment is required, and the fluence should result in epidermal whitening without vesiculation or pin-point bleeding. A single pass is typically performed, but pulses may be stacked over macular seborrheic keratoses.
In a study comparing three lasers and liquid nitrogen (Medlite II frequency-doubled QS Nd:YAG laser, Continuum Biomedical, Livermore, CA; HGM K1 krypton laser, HGM Medical Laser Systems Inc., Salt Lake City UT; DioLite 532-nm diode-pumped vanadare laser, Iridex Corp, Mountain View, CA), a single treatment with the frequencydoubled QS Nd:YAG laser was the most effective agent at destroying melanin and preserving the surrounding tissue.58
For QS and picosecond lasers, patients should be counseled that they may see urticarial-like papules for 24 hours followed by 7 to 10 days of purpura or coffeeground appearing macules, followed by temporary hypopigmented macules, which can be seen after the lesion sloughs superficially (Table 80-5). Purpura is more frequently encountered with the QS Nd:YAG (532 nm) or pulsed-dye lasers because the competing chromophore, deoxyhemoglobin, causes immediate rupture of small vessels.53 The use of the QS ruby laser is not recommended in darker skin types. These can be more safely treated with the 1,064-nm QS or picosecond Nd:YAG laser.37
IPL therapy has been used as a nonablative photorejuvenating device for the hand. IPL systems are high-intensity pulsed sources emitting light between 515 and 1,200 nm. This broad spectrum facilitates the selective targets of vessels with hemoglobin (580 nm), or deoxyhemoglobin and melanin (400–755 nm). Its largest advantage is that it allows simultaneous correction of vascular and pigmented lesions with little to no downtime.59 Additionally, dermal heating from IPL therapy, which spares the epidermis, has been shown histologically to induce collagen production in the papillary and reticular dermis.60 Filters can be added to select for wavelengths only above a certain range. Fitzpatrick skin types IV to VI require cut-off filters at higher wavelengths, triple pulsing and longer pulse delays between pulses in order to prevent damage or epidermal compromise (Table 80-6). Optimal correction of erythema and vascular lesions, where oxygenated hemoglobin predominates, can be achieved using 515- to 590-nm cut-off filters (based on patient skin type and extent of erythema). Purpuric patches (rich in deoxygenated hemoglobin) are better targeted with filters of 590 nm or higher.
Settings using the Lumenis 1 or the Lumenis M22 IPL (Lumenis Ltd., Yokneam, Israel) are optimized with a 560-nm cut-off filter for skin types I to III and a 590-nm filter for skin type IV, is used. Patients with predominantly mottled hyperpigmentation and solar lentigines benefit from a double-pulse technique with a 3-ms pulse duration. If there is a combination of pigment and vascular structures, a 3.5-ms pulse duration for
both pulses is used, and a 4-ms pulse duration is used if only fine telangiectasias and erythema predominante. A 10- to 30-ms delay is set between pulses in skin types I to III and a 30- to 40-ms delay in skin type IV. The fluence is set between 15 and 18 J/cm2. Treatments are performed monthly for two or three sessions.
In a study by Goldman, 23 patients with dermatoheliosis and solar lentigines on the dorsal hands were treated with four IPL sessions at 3- to 4-week intervals.61 In 100% of cases, investigators noted good to excellent results in the improvement of lentigines and skin quality. Subjective patient self-assessments showed similar results. Twenty of 23 (87%) of subjects noted good to excellent improvement. No significant side effects were observed (Fig. 80-9).
PDT is an effective photoaging treatment, especially in the presence of precancerous conditions. PDT uses a photosensitizer, such as 20% aminolevulinic acid (ALA) solution or 16% methyl aminolevulinate (MAL) cream, which is converted in vivo into protoporphyrin IX. PDT is indicated for the treatment of nonhyperkeratotic actinic keratoses, with the advantageous side effect of improving the appearance of fine lines and rhytides, mottled hyperpigmentation, and texture.53 To increase efficacy from a single PDT treatment, patients may apply other topicals (imiquimod or 5-fluorouracil) for 7 to 10 days prior to PDT treatment to the area to be treated. ALA or MAL may be applied after the dorsal hand skin has been exfoliated with a vibrating microdermabrasion system (if available) and degreased with an acetone wash. On the hands, photosensitizer may be left in place for 3 hours occluded, and ideally under a warming blanket or in a warm dimly-lit room. After the photosensitizer has been washed off with soap and water, and a baby wipe has been used to remove any additional residue, any light source within the visible light spectrum can be used to activate the photosensitizer. Friedman et al. found a sequential combination of laser and light sources to be superior to using a single light source.62
The sequence is as follows: initial activation with a PDL (Cynergy, Cynosure, Westford, MA) 595 nm with a 7 mm spot size, 40-ms pulse width, and 10 to 12 J/cm2 targeting individual actinic keratoses so that the endpoint is subpurpuric. This is followed by the IPL using the treatment parameters outlined above. Finally, the treatment area is concomitantly illuminated with a blue light source (Blu-U, DUSA Pharmaceuticals, Inc., Wilmington, MA) positioned 25 to 50 mm from the skin for an illumination period of 16 minutes 40 seconds, light dose 10 J/cm2 and a red light source (Aktilite CL 128, PhotoCure ASA, Oslo, Norway) positioned 50 to 80 mm from the skin for a total of 8 minutes, 49 seconds at a standardized fluence of 37 J/cm2. Prior to discharge home, a mineral-based sunscreen is applied and the patient is told to stay indoors with strict sunlight avoidance for the remainder of the treatment day and the following day. Using this combination, generally one PDT treatment is sufficient. Orringer et al. examined the histologic effects of PDT on the hand and found an increase in expression of procollagen types I and III, epidermal thickening, and an increase in Ki-67, a keratinocyte differentiation marker, after PDT using a 595-nm PDL for activation of the photosensitizer.63
Nonablative laser resurfacing also improves the appearance of photodamaged skin of the hand. These lasers emit longer wavelengths, in the mid-infrared range, that penetrate into the deep dermis, stimulating fibroblasts while avoiding injury to the epidermis.
The 1,320-nm Nd:YAG laser been employed as a treatment modality in hand rejuvenation. Sadick and Schecter performed a study involving seven patients using the 1,320-nm Nd:YAG laser (CoolToughII, New Star Lasers, Roseville, CA, USA).64 These patients received six treatments separated by 4 weeks and were followed for 3 months after the last treatment. Patient assessment scores were higher than objective measures, with six of seven patients reporting a mean improvement score of 2 (range 1–6), corresponding to 1% to 19% improvement from baseline. Results are mild to moderate at best, and patients should be warned of the slow progress and subtle improvement that can be expected.
Nonablative fractional lasers treat a fraction of the skin as compared with traditional nonablative lasers, leaving up to a maximum of 95% of the skin uninvolved. Microthermal treatment zones (MTZs) are delivered to the dermis, causing coagulation necrosis followed by collagen remodeling. The selected wavelength should correspond to the cosmetic target; the 1,550-nm wavelength is best for stimulating collagen production and improving skin texture, while the 1,927-nm wavelength and 1,927-nm thulium lasers are best for pigmentation (Table 80-7).65 Jih et al. employed fractional resurfacing technology for hand rejuvenation using the 1,550-nm diode-pumped erbium fiber laser (Fraxel SR, Reliant Technologies) on a series of 10 patients.66 Patients received a total of 5 treatments 2 to 3 weeks apart using a setting of 8 to 9 mJ/MTZ with 10 passes at 250 MTZ/cm2 to achieve a final treatment density of 2,500 MTZ/cm2. The
study reported a subjective patient improvement of 51% to 75% in skin pigmentation and 25% to 50% improvement in skin roughness and wrinkling. Biopsies of the skin showed an increase in density of dermal collagen. It may be best to use one wavelength per session to allow a more focused treatment and include a greater number of passes.
Ablative laser skin resurfacing using the CO2 or Er:YAG laser is the standard for facial rejuvenation. When employing this modality for hand rejuvenation, great caution should be taken because of the reduced number of pilosebaceous structures and vasculature. This leads to a lengthier recovery period, a higher risk of infection, and a greater risk for scarring and dyschromia. Optimal treatment parameters using the Er:YAG laser that have been reported in the literature include the use of two passes at 15 J/cm2 and 30% intensity, followed by cleaning and a third pass at the same settings.53 A single-pass resurfacing technique has also been described using decreased fluence (150–200 mJ/pulse) with a computer-generated pattern of 6, leaving the epidermal debris in place to serve as a biologic dressing.1
Fractional thermolysis can also be employed by ablative fractional lasers. This creates columns of vaporized tissue and coagulation necrosis. Because only a small portion of the skin is affected, neighboring untreated tissue aids in the healing process promoting a favorable side-effect profile and minimal posttreatment recovery. Stebbins et al. treated the hand with a single-pass of the Dermal Optical Thermolysis ablative fractional CO2 laser (DEKA, Calenzano, Italy) and noted transient erythema and edema, with no long-term scarring or pigmentary alterations.67 After three treatments at 4- to 6- week intervals, investigators rated a mean improvement of 26% to 50% for wrinkles, 51% to 75% for pigment, and 26% to 50% for texture, with subjects reporting similar results.
Pretreatment, a topical anesthetic such as bupivacaine/lidocaine/tetracaine anesthetic cream is applied for 30 minutes preoperatively.53 After the removal of the cream, the area is treated with a nonsequential fractional CO2 laser using 75-mJ, 100-Hz, and a 0.3-second repeat delay (Active FX, Lumenis Ltd., Yokneam, Israel). A computer pattern generator with settings of 3 pattern, 5 size, and 1 density (corresponding to less than 10% overlap) is used. After the procedure, cool sterile saline compresses and ointment are applied. In skin types III or greater, a class VI topical corticosteroid ointment is started daily for 5 days on postoperative day 2 to minimize the occurrence of
postinflammatory pigmentary alteration. The use of fractionated ablative laser is generally not recommended in patients of skin types V and VI unless performed by a highly experienced laser surgeon (Fig. 80-10).
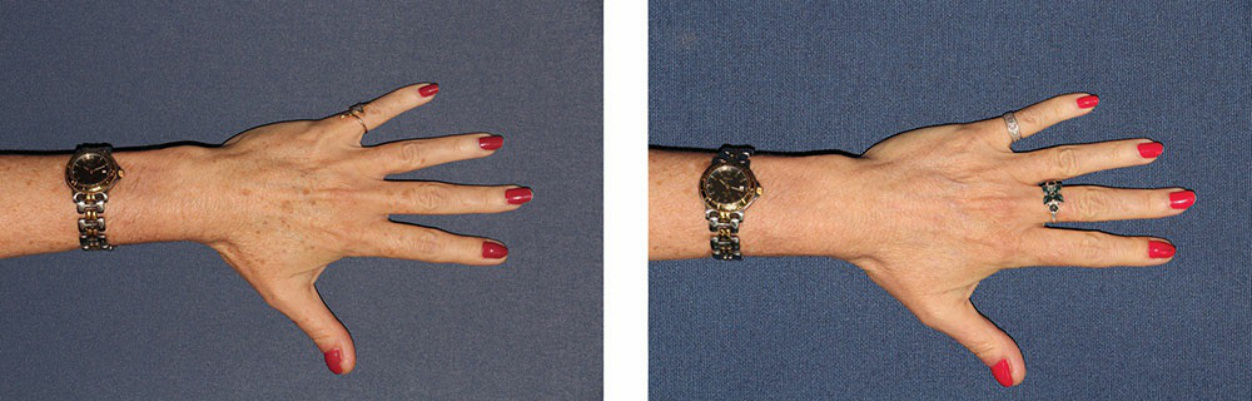
Figure 80-9. A 57-year-old patient presented with fine wrinkling, solar lentigines, and macular seborrheic keratoses of the dorsal hands and digits. She underwent one session of intense pulsed light and Q-switched alexandrite to the hands, with improvement in texture and pigmentation. Before (left) and 4 weeks after (right) one session of intense pulsed light and Q-switched alexandrite to the hands.
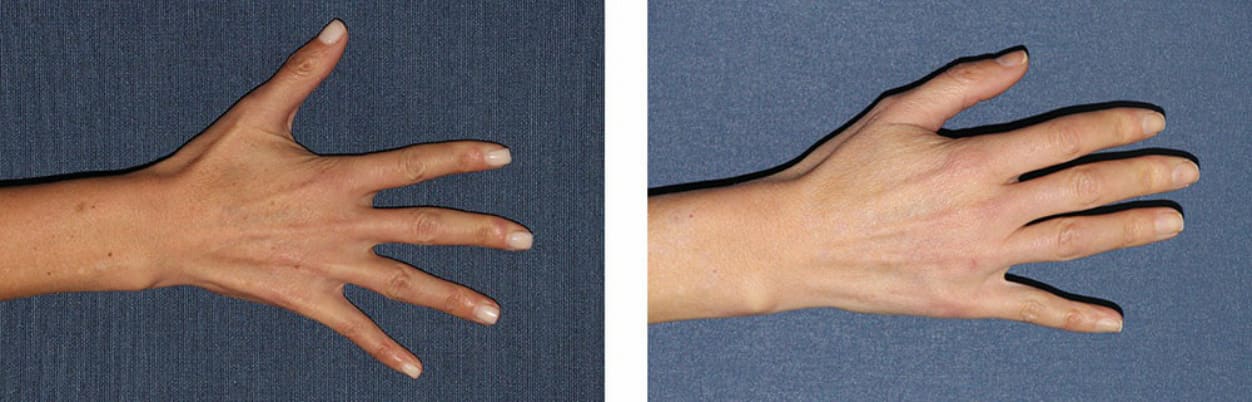
Figure 80-10. A 42-year-old female demonstrated scattered and few solar lentigines and macular seborrheic keratosis on the dorsal hand. One treatment of Q-switched alexandrite to the lesions resulted in complete clearance of the lesions. Before (left) and 7 weeks after (right) one treatment of Q-switched alexandrite.
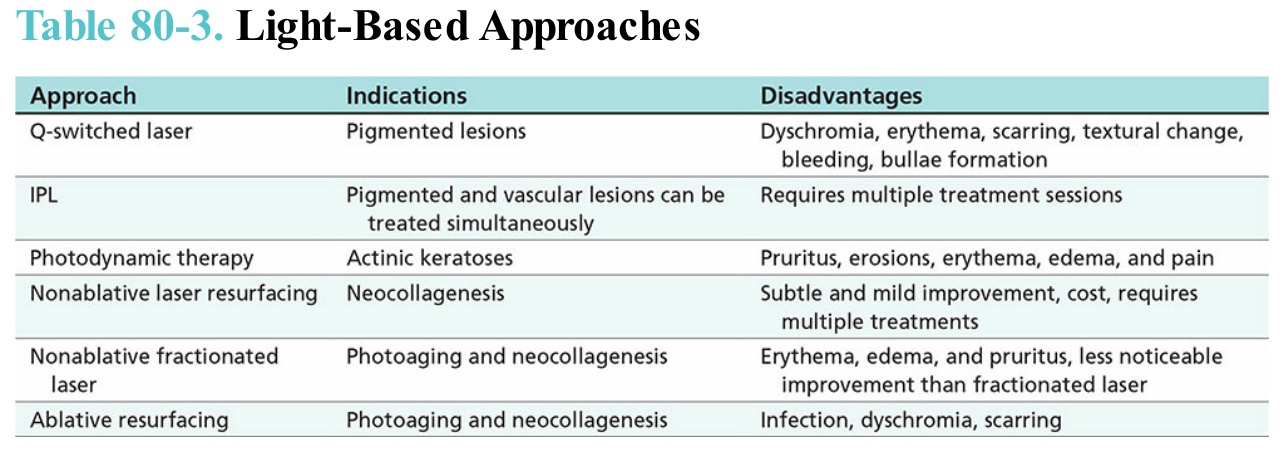
Table 80-3. Light-Based Approaches
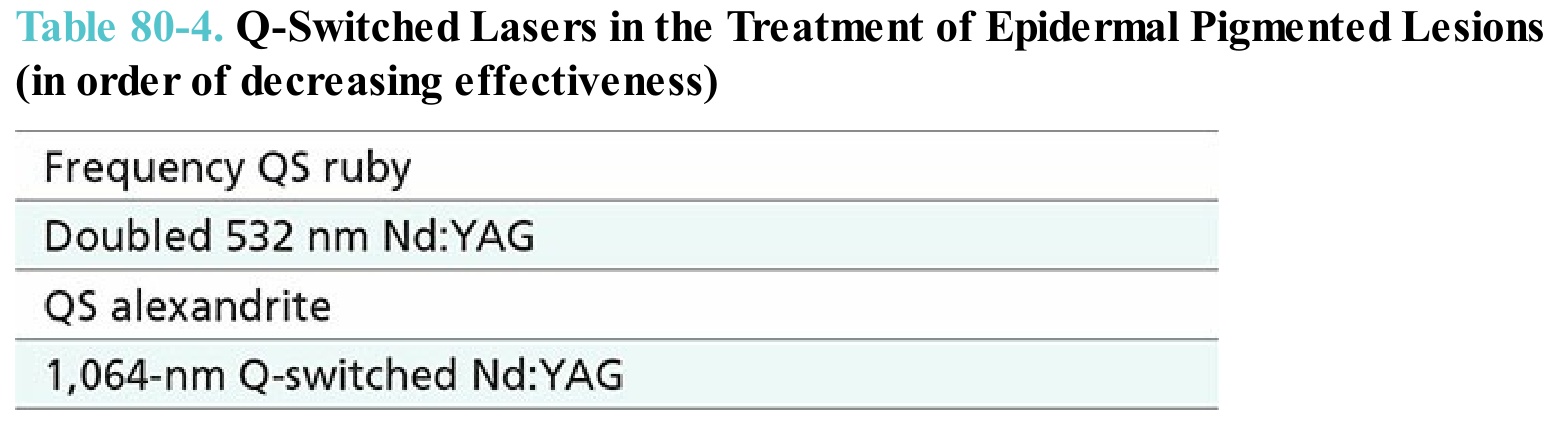
Table 80-4. Q-Switched Lasers in the Treatment of Epidermal Pigmented Lesions (in order of decreasing effectiveness)
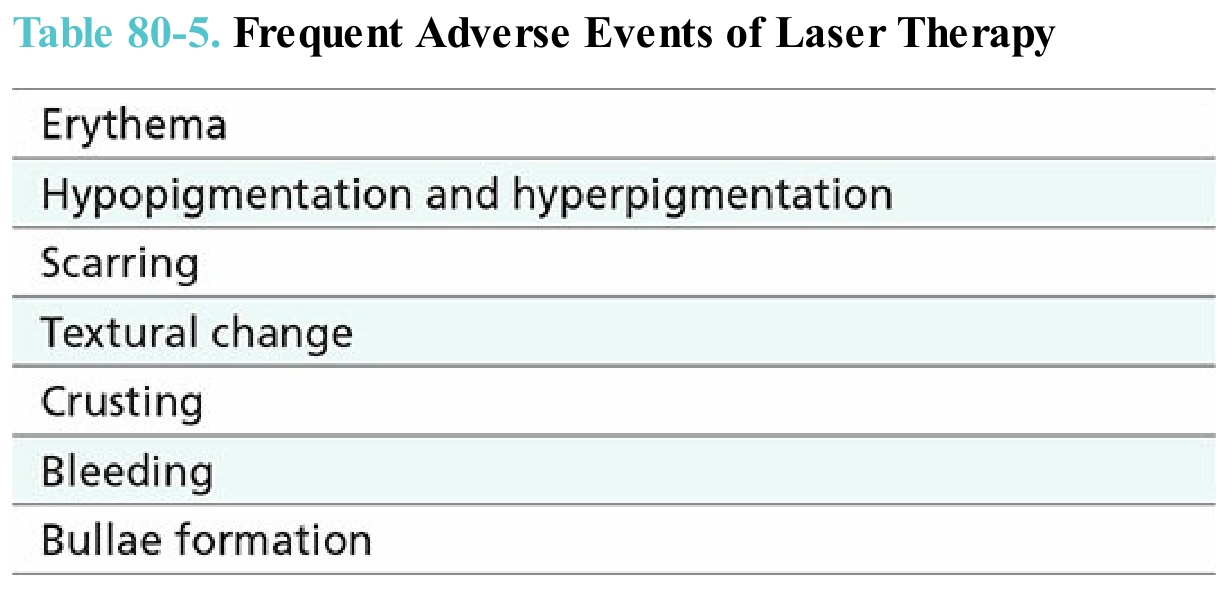
Table 80-5. Frequent Adverse Events of Laser Therapy
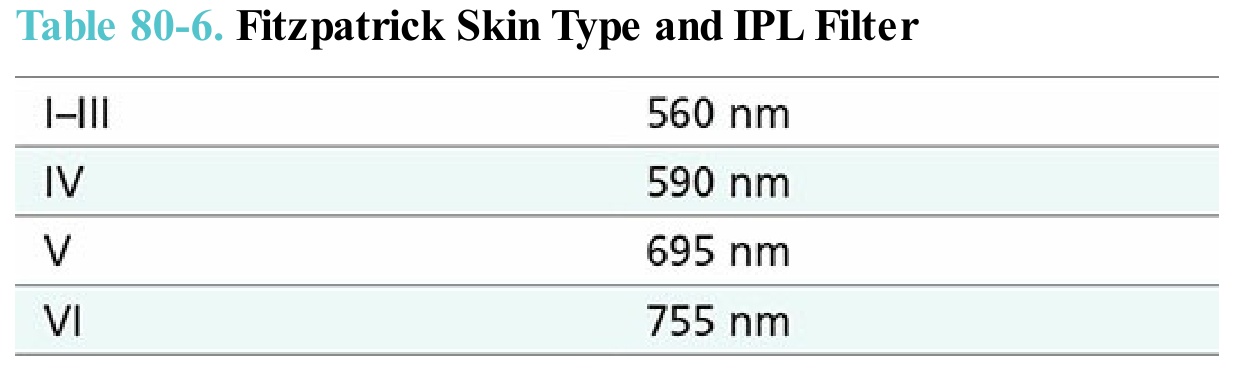
Table 80-6. Fitzpatrick Skin Type and IPL Filter

Table 80-7. Common Settings for Nonablative Fractional Laser