Sclerotherapy
Sclerotherapy
In sclerotherapy, a liquid or foam is injected into a vein in order to produce endothelial cell damage and resultant vessel sclerosis. Various agents can be used to perform sclerotherapy. On the hand, the detergents sodium tetradecyl sulfate (STS) (Sotradecol Elkins-Sin, Inc., Cherry Hill, NJ) and polidocanol (POL) (Asclera; Kreussler, Chemische-Fabrik, Wiesbaden, Germany) are most commonly used. Both are FDA approved for small varicosities of the lower extremity. Thus, their use on dorsal hand veins is off-label.
Good candidates for sclerotherapy are patients with bulging dorsal hand veins who do not have known contraindications to sclerotherapy. For the hands specifically, sclerotherapy should be avoided in patients with a history of hand surgery, need for frequent intravenous access, hand arthritis, chronic edema or pain of the hands, functional abnormalities of the hands, carpal tunnel syndrome, or dialysis shunts.10
Prior to starting the treatment session, the patient is seated with the arms positioned perpendicular to the upper body. The entire hand and wrist are prepped with chlorhexidine. A tourniquet, or pressure from an assistant’s hand, is applied to the midforearm in order to increase the prominence of the veins, making them easier to inject.
Concentrations of 0.5% to 3% liquid STS or 1.5% to 3% liquid POL are most commonly used. In general, lower concentrations should be used for smaller veins, and higher concentrations for larger veins. Duffy et al. treated 100 patients with dorsal hand veins ranging from 1 to 6 mm in diameter (mean of 3 mm) with liquid 0.5% STS, 1.5% POL, or 3% POL.45 They observed higher success rates in patients treated with 3% POL (95% vs. 20% success rate). The authors concluded that 3% POL is more effective in
vessels larger than 3 mm, or vessels of any diameter in younger patients. It is important to note that 14.5% of the patients treated with 3% POL developed telangiectatic matting in the treatment area, a side effect which was not observed with 0.5% STS or 1.5% POL. Bowes et al. reported complete resolution of 3 to 6 mm dorsal hand veins in 11 of 14 (79%) hands treated with 1 to 4 mL of liquid 1.5% to 3% STS.46
With foam sclerotherapy, the sclerosing solution is mixed with either room air or carbon dioxide (CO2) gas. Foaming allows for longer contact between the sclerosant and the endothelium, increasing the efficacy of the procedure and allowing the physician to use lower concentrations and smaller volumes of sclerosant.47 Rao et al. attach a 3- mL syringe filled with 1 mL of the sclerosant to a 5-mL syringe containing 4 mL of room air. A female-to-female connector is used to attach the two syringes. The liquid and room air are mixed together approximately 10 times until a homogeneous consistency is achieved. Either 0.5% STS or 1% POL, with a total of 3 to 5 mL of foamed sclerosant per hand, is frequently used.21 In a retrospective review of 38 hands, Tremaine et al. used 2.5 to 10 mL of foamed 0.25% to 1% STS per hand, with 0.5% and 0.25% predominating.10
For practical purposes a single hand is treated per day, generally using a 30-G, 0.5- in needle connected to a 3-mL syringe of sclerosant. The vein should be entered at its most distal aspect and canalized in a proximal direction. With the bevel of the needle facing up, the vein is directly punctured, entering at an angle of 30 to 45 degrees to the skin. The sclerosant is injected slowly. Once all the desired vessels are treated, the tourniquet is released, the hand is elevated, and gentle massage is performed to the treated area from a distal to proximal direction. Cotton swabs are then applied to each treatment site, and the hand and distal forearm are wrapped in an elastic bandage. The patient is asked to keep the bandage on for 24 hours, and can return for treatment of the second hand the following day so that the other hand is free to assist with daily function. Signs of excessive compression from the bandage include paresthesias, decreased motion, or changes in temperature or color of the fingers. Some authors recommend keeping continued compression for 2 weeks.48
Common side effects due to sclerotherapy include pain during the injection, ecchymosis, edema, and soreness. Tremaine et al. noted pain lasted an average of 7.4 days, edema and erythema 3 to 4 days, and ecchymosis 3.7 days.10 Less frequently, patients may developed hyperpigmentation, neovascularization, localized hypertrichosis (never reported in the hands), urticaria, and allergic reactions. In their study, Tremaine reported that 61.9% of 38 treated hands developed posttreatment coagulum. A 22-G needle can be used to pierce the center of the coagulum, and its contents can be gently expressed; all coagula in the study resolved within 2 months. Patients should be seen for follow-up at 2 weeks to assess for this complication. Neovascularization, or telangiectatic matting, more often occurs in patients with high levels of estrogen, as seen
during pregnancy and the use of oral contraceptives or estrogen supplementation.49,50 High volume of sclerosant, high injection pressure, large treatment areas, extensive blanching upon injection, and lack of posttreatment compression are also associated with the development of neovascularization.50,51
Rare adverse events include local skin necrosis, arterial injection resulting in distal skin necrosis, thrombophlebitis, DVT, wheezing in asthmatics, and angina in cardiac patients.52 Duffy et al. reported one patient who, after treatment of vessels located on the thenar web, developed blanching of the thumb, index, and middle finger for 10 minutes.45 The patient then experienced 2 weeks of numbness and paresthesia. These symptoms were thought to be secondary to neuropraxia caused by extravasation of the sclerosing agent. Although never reported in treatment of the dorsal hand, the microbubbles introduced into the circulation by foam sclerotherapy can cause visual changes, headache, chest tightness, coughing, migraine with or without aura, and transient ischemic attacks (Fig. 80-8).
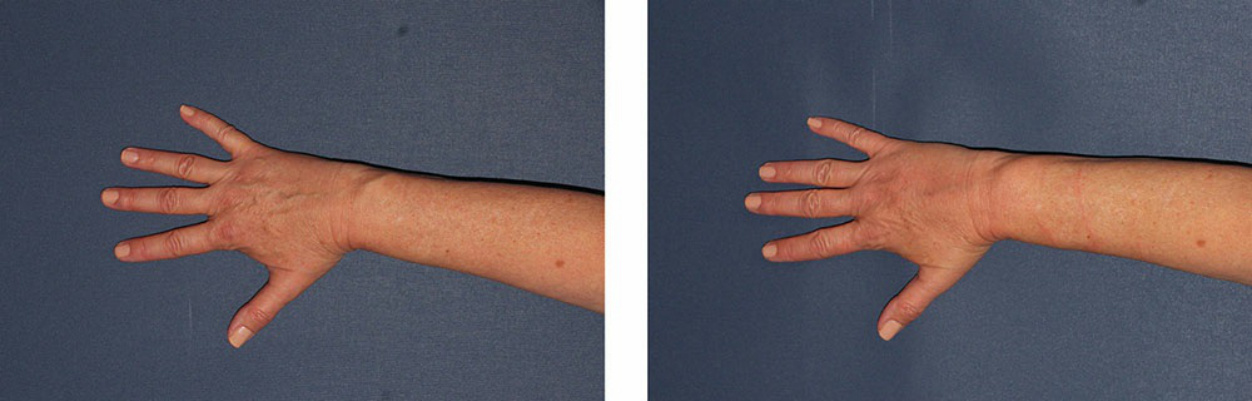
Figure 80-8. A patient was extremely bothered by her prominent hand veins. She had no history of diabetes or kidney disease, and denied need for frequent IV access. The patient did not want to have any fillers injected, and was not bothered by prominent tendons or the quality of skin. She subsequently underwent sclerotherapy. Before (left) and 24 hours post (right) foam sclerotherapy to the dorsal hand.