Hyaluronic acid
Hyaluronic acid
HA, a naturally occurring glycosaminoglycan, can also be used for hand rejuvenation. Man et al. and Brandt et al. demonstrated the efficacy of Restylane® (Medicis Aesthetics Inc., Scottsdale, AZ), a small gel-particle (SGP) non–animal-derived stabilized (NASHA) made of 20 mg of HA per mL, for volume augmentation in a total of 48 patients (10 and 38, respectively).25,26 In their study, Man et al. compared 2 vials of SGP-NASHA to 2 vials of human collagen. With the patient in Trendelenburg position, filler was injected subcutaneously, inserting the needle at an oblique angle adjacent to the dorsal hand veins. Gentle massage was then performed with the hand in a flexed position. HA was found to be more painful (likely due to the presence of lidocaine in human collagen), but produced greater patient satisfaction; it was also more efficacious at improving the physician-assessed visibility of dorsal hand veins. In order to decrease pain during massage, NASHA can be premixed with lidocaine.21
SGP-NASHA (20 mg/mL) was used on 16 patients by Brandt et al.26 This study found substantial improvement in the prominence of vessels, tendons, and bones, in skin turgor, and in patient and investigator global aesthetic improvement and satisfaction scales. Using a single entry point, the material was threaded along the dorsum of the hand. The authors did not indicate whether a needle or cannula was used. The mean volume used for both hands was 7.38 mL, with a maximum of 4 mL per hand. Five patients underwent a touch-up treatment at 2 weeks, using a mean volume of 1.96 mL for both hands.
A European study treated 99 patients with Juvéderm® (Allergan, Inc., Irvine, CA, USA).27 Juvéderm Ultra 3, with volume of 0.8 to 1.6 mL, was injected into the mid to deep dermis at the first visit. Injections were performed via cannula in 54.3% of patients, and the rest through needle. Juvéderm Hydrate, with a volume of 0.5 to 1.0 mL was injected into the superficial dermis at day 15. Injections were performed via needle in 79.3%, and the rest through cannula. The study demonstrated a significant improvement in patient and investigator assessments. Interestingly, the proportion of injections rated as “very easy” was significantly higher with needle for Juvéderm Ultra 3, than with cannula for Juvéderm Hydrate. Edema, hematoma, redness, and pain were experienced by 13.2% of patients. Of these 32 adverse events, 26 were reported with cannula and 6 with needle. Additionally, subject discomfort was found to be significantly greater with cannula injections (Fig. 80-7).
Another study compared 27-G hypodermic needles to blunt-tipped microcannulas (using either a 25-G 50-mm flexible microcannula or 18-G 70-mm semi-rigid microcannula) on the dorsal hands.28 A total of 95 patients were injected with 20 to 28 mg/mL of HA. In both methods, the filler was placed in a linear retrograde fanning technique. The authors found that while there was no difference in the GAIS score between the two techniques, pain and bruising were greater with the use of a hypodermic needle.
In a placebo-controlled study, Gubanova et al. utilized a multipuncture, microinjection technique to assess NASHA versus saline in 30 patients.23 A 30-G needle was introduced 3 to 4 mm into the dermal layer, delivering 0.02 mL of product. Approximately 50 injections were placed at even intervals along the dorsal hand until the desired outcome was achieved. Patients received 1.0 mL of HA or 1.0 mL of saline monthly, for a total of three treatments. HA showed a significant improvement in patient and investigator questionnaires and measurements of skin hydration and elasticity.
Restylane® Vital® or Vital Light® (Q-med, Uppsala, Sweden) have been used for hand rejuvenation in parts of Europe and Asia. Unlike other Restylane products, Restylane Vital contains 12 mg/mL of HA. Streker et al. employed the Restylane®
Injector® (Q-Med AB, Uppsala, Sweden) to deliver a controlled volume of 10 μL per injection into the mid dermis, using a 30-G needle.29 Injections were spaced 0.5 to 1.0 cm apart. A mean of 2.8 mL of NASHA was injected per hand. All patients demonstrated aesthetic improvement and increased satisfaction through the 36-week follow-up. Lacarrubba et al. also applied an autoinjector to dispense aliquots of approximately 17 μL of either 16 or 20 mg/mL HA salts (Viscoderm; Bigpharma, Seixal, Portugal) per injection.30 Each hand received 30 microdroplets at a maximum volume of 1.0 mL. Patients received treatment every week for 4 weeks. Ultrasound was performed prior to each treatment and 1 week following the fourth injection. Fifteen of 19 subjects
demonstrated a statistically significant increase in subepidermal low-echogenic band echogenicity, which the authors believed to represent an increased density of collagen fibers produced by activated fibroblasts.
Side effects of HA injection in these studies included pain, edema, and ecchymosis. The results produced by HA are expected to last 6 to 12 months.21 HA has the advantage of being reversible with hyaluronidase. However, it has a shorter duration, requires more syringes per hand to achieve a significant improvement, and has the potential for causing the Tyndall effect if placed too superficially; no studies have reported Tyndall effect with the use of HA on the hands.
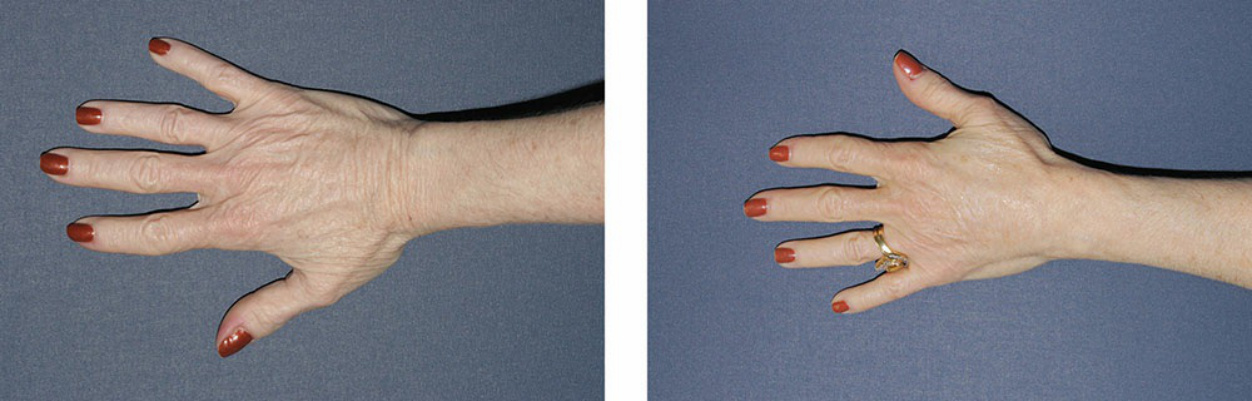
Figure 80-7. Fat transfer to the hands was elected to restore volume to the patient’s hands as she was already planning to undergo liposculpture. Otherwise, CaHA would have been the filler of choice to avoid undergoing a costly harvesting procedure that adds a different set of side effects from simply using a synthetic filler. Before (left) and 30 days after (right) 8 mL of autologous fat to the dorsal hand.