Calcium hydroxyapatite
Calcium hydroxyapatite
Calcium hydroxyapatite (CaHA), or Radiesse® (Merz Aesthetics, Franksville, WI), is the only dermal filler approved by the United States Food and Drug Administration (FDA) for hand rejuvenation. CaHA microspheres, which are made of substances identical to human bone, are suspended in a polysaccharide carrier made of glycerin and sodium carboxymethylcellulose. This filler is biodegradable (broken down into calcium and phosphate over time) and biostimulatory (stimulates collagen deposition by fibroblasts) (Fig. 80-5).
her prominent veins, and wants sclerotherapy of her hands. Upon inspection, it was noted the patient had prominent dorsal hand tendons in addition to veins. Patients are always encouraged to restore dorsal hand volume prior to treating veins alone. Adding volume to the dorsal hands typically minimizes the appearance of the prominent veins while also addressing tendons and improving the quality of skin. Using 1.5 mL of CaHA diluted with 0.5 mL of lidocaine, 1.0 mL of product was injected into each hand. When injecting, it is important to remember that the safest plane of filler injection is the potential space between the dermis and superficial fascia. This plane can be accessed via the scrape skin threating technique. Before (left) and 14 weeks after (right) 1.5 mL of CaHA mixed with 0.5 mL of lidocaine, 1.0 mL to each hand.
Three prospective, randomized, controlled clinical trials in the United States, Germany, and Canada between 2008 and 2014 and involving a total of 256 patients led to the approval of Radiesse for hand rejuvenation.17 Using either the MHGS or BHVSS, 66% to 100% of patients achieved at least a one-point decrease in their grading score. Multiple other studies dating to 2007, involving over 100 patients, have demonstrated the efficacy of CaHA for dorsal hand rejuvenation. When used on the dorsal hand, CaHA has been shown to last 12 to 24 months.18–21
Previously published literature has reported the use of different dilutions, filler volume, and injection techniques. Overall, dilution of CaHA with lidocaine or saline reduces the viscosity and facilitates an even distribution of the filler.21 Additionally, lidocaine makes the procedure more comfortable for the patient. The various options for injection include the bolus method, linear retrograde, fanning, serial puncture, microdroplets, and cannula.
In the pivotal U.S. trial, no more than two syringes of product were used per hand (1 syringe = 1.5 cc of CaHA mixed with 0.26 cc of 2% lidocaine).16 Using a 27-G needle, boluses of up to 0.5 cc were introduced via a skin tenting technique, in the area bounded by the first and fifth metacarpals, dorsal wrist crease, and MCP joints.11 The needle is inserted parallel to the bone, and a bolus is placed within the center of the tented skin.11 The bolus is thoroughly massaged into the areas of volume loss until an even surface is achieved. Massage is most easily performed with the hand in a flexed position. Topicals such as emollients, hand soap, chlorhexidine, ultrasound gel, and vitamin K cream may aid in the massage.3
Busso and Applebaum, in the first trial to examine CaHA for hand rejuvenation, used a 1.3 mL vial of CaHA mixed with 0.1 mL of plain 2% lidocaine per hand.22 The syringe of CaHA is attached to a 1-mL syringe of lidocaine using a Rapid Fill™ Luer- Lok-to-Luer-Lok connector (Baxa; Englewood, CO), and the solutions are mixed back and forth until a homogeneous consistency is achieved. A bolus of 0.5 to 1.4 mL was introduced through a needle into the areolar plane between the subcutaneous layer and superficial fascia. Fabi and Goldman in 2012 described their technique of using a 1.5 mL vial of CaHA mixed with 0.3 mL of plain 1% lidocaine and 1.2 mL of bacteriostatic 0.9% sodium chloride in a 1:1 dilution.21 After injecting a bolus, similar to Busso and
Applebaum, vigorous massage is performed with the assistance of a soapy cleanser.
In their anatomical study, Lefebvre-Vilardabo et al. concluded that the safest plane to inject would be the potential space between the dermis and superficial fascia, away from veins and tendons.11 In order to compare the placement of filler using different injections techniques, the authors performed an MRI after injecting CaHA into cadaveric hands. Single bolus of 1 mL using a 21-G needle, single bolus plus massage, blind retrograde threading of 0.8 mL of CaHA using a 27-G cannula, and scrape skin threading technique (SSTT) of 0.7 mL of CaHA using a 21-G cannula were compared. In all techniques except SSTT, MRI showed product in the deep fascia and surrounding tendons. Although this placement of filler in the subdermal plane seems ideal, little is known about the actual consequences of the presence of filler material in deeper planes.
In SSTT, a soft tip blunt 21- or 23-G cannula is used. First, a needle slightly larger than the cannula creates an entry point in the web space between the MCPs. Next, the cannula is inserted through the entry point with the bevel facing up toward the dermis. The cannula is gently guided toward the wrist; the injector should feel the cannula scraping the underside of the dermis. Then, filler can be slowly and evenly injected as the cannula is withdrawn. The cannula can then be repositioned through the entry point and a fan-shaped configuration used to fill the triangular area of volume loss corresponding to the interosseous spaces. If necessary, additional entry points can be made and the same technique used to fill more proximal areas of volume loss. Gentle massage is used to correct unevenness. This approach may also be used with entry points on the proximal hand near the hand–wrist crease, pointing the cannula toward the MCPs.
In a 2015 study, Gubanova et al. compared a multipoint technique using a needle to a fan-like technique using a cannula.23 CaHA 0.8 mL with 0.2 mL of 2% lidocaine was used for each injection method. In one hand, a 27-G needle was used to inject 0.025 mL of product into multiple sites. On the other hand, a 25-G, 50-mm blunt cannula was used to distribute filler in a fan-like distribution in the upper subdermal layer. Both techniques resulted in similar response rates, satisfaction scores, and adverse events, all of which were mild (Fig. 80-6).
On occasion, a patient may also desire volume correction of the space between the MCPs and PIPs. Lefebvre-Vilardabo et al. recommend injecting only dorsally between the MCP and PIP, and avoiding injecting over the joint or laterally as the arteries and veins run on both sides of the digit. After injection, the filler can be blended with the hand in palmarflexion.11
The expected adverse events of CaHA injection include transient edema, erythema, pain, and ecchymosis lasting up to 2 weeks. In the pivotal trials, pain and edema were the most common adverse events, with 89% of symptoms developing within 14 days.17 Seven (6.2%) of the patients developed palpable nodules, all of which resolved without intervention by day 268. In certain cases, the onset of swelling can be delayed by 30 days. Busso et al. note that CaHA mixed with lidocaine can produce more prominent edema than using undiluted CaHA.16 Ice, hand elevation, gentle compression, and light massage can help reduce the edema. Another study evaluated the use of triamcinolone to minimize adverse events associated with CaHA injections.24 Twenty subjects were injected with 1 syringe of CaHA diluted with 0.3 mL of 1% lidocaine and 1.2 mL of bacteriostatic normal saline. Following treatment, each hand was randomized to receive injections of either 5 mL of 2 mg/mL triamcinolone acetate or 5 mL of bacteriostatic normal saline. A blinded investigator noted a decrease in edema at days 7 and 14 postinjection in the triamcinolone-treated hands (p < 0.10). This was corroborated by a
statistically significant increase in swelling from days 6 to 19 in the placebo hand, documented in the subjects’ daily diary. No statistically significant difference in treatment efficacy was noted between those treated with triamcinolone or placebo.
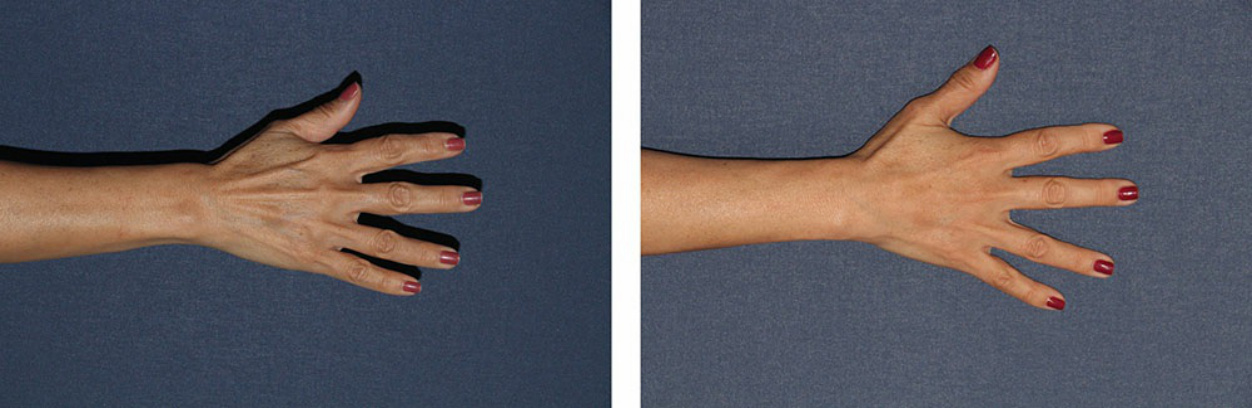
Figure 80-5. A 58-year-old female presented to clinic worried about the aged appearance of the hands, specifically

Figure 80-6. A 66-year-old female had CaHA injections using two techniques. One hand was injected with 1.5 mL of CaHA diluted with 0.5 mL of 1% lidocaine, using a 1.5-in 25-G blunt-tipped cannula and a linear threading technique. The other hand was injected with 1.5 mL of CaHA diluted with 1.5 mL of bacteriostatic normal saline, using a 1.0-in 27-G cannula and a multiple bolus technique.