HAND ANATOMY
HAND ANATOMY
The hand fulfills multiple purposes, including sensation, movement, and communication.7 It is able to achieve these functions via a complex network of bones, muscles, nerves, ligaments, tendons, arteries and veins. When performing hand rejuvenation procedures, one should be familiar with the relevant anatomy of the dorsal hand.
The external anatomy of the hand is pictured in Figure 80-1. In the anatomic position, palmar (volar) refers to the anterior surface of the hands, while dorsal refers to the posterior surface of the hand. In order to indicate laterality, most physicians use the terms ulnar and radial.
The median, radial, and ulnar nerves supply both the motor and sensory innervation to the hand and digits.8 The radial nerve supplies the sensory innervation to the radial dorsal hand, and the ulnar nerve to the ulnar dorsal hand (Fig. 80-2). The blood supply of the hand originates from the radial and ulnar artery.9 The palmar hand contains the superficial and deep palmar arteries, which give off various digital arteries. In the dorsal hand, branches of the radial and ulnar artery form the dorsal carpal arch, which is located within the dorsal wrist below the thick fascia of the extensor retinaculum. From the dorsal carpal arch come the dorsal metacarpal arteries, which travel in close proximity to the muscles and bones of the dorsal hand. Eventually dorsal digital arteries branch from the dorsal metacarpal arteries.
There are three venous systems in the hand: the superficial palmar veins, deep palmar veins, and dorsal venous arch.10 Valves within these veins direct most of the blood flow to the dorsal vein, which then courses into the basilic vein (ulnar side) and cephalic vein (radial side). Because of various communications and redundancy between these systems, obliteration of the dorsal hand veins does not impair venous drainage.4
In the anatomic snuffbox, the radial artery, cephalic vein, and superficial branch of the radial nerve sit above the scaphoid and trapezium bones (Fig. 80-1). Filler or sclerotherapy injections into this area should be avoided because of the risk of canalizing or injuring these important neurovascular structures.
The skin of the dorsal hand is thin and has few appendages, resulting in inferior wound healing compared to other parts of the body. It is also more loosely connected to the underlying structures. Lefebvre-Vilardabo et al. conducted an in-depth review of the anatomy of the dorsal hands through cadaveric dissection and duplex ultrasound, studying live subjects ranging in age from 25 to 72.11 They found that the dorsal hand is composed of the epidermis, followed by the dermis, sponge-like fascial layer, tendons, deep fascia, and bones with their interosseous muscles (Fig. 80-3). The dermis measured 0.2 to 0.9 mm, the fascial plane 0.3 to 2.2 mm, and the tendon layer 0.7 to 1.7 mm. They found an intricate pattern of veins residing at all levels of the fascial layer. It is therefore important to keep in mind that the bevel of a needle is 0.75 mm in length.
Another anatomical study by Bidic et al. used histologic analysis, duplex ultrasonography, and lead oxide evaluation to examine the dorsal hand.12 They found three separate fat compartments and fascial layers. From superficial to deep, the authors observed the epidermis, dermis, dorsal superficial lamina, dorsal superficial fascia, dorsal intermediate lamina, dorsal intermediate fascia, dorsal deep lamina, dorsal deep fascia, followed by muscles and tendons. Since veins were found in the dorsal intermediate lamina and extensor tendons in the dorsal deep lamina, the authors concluded the safest plane of injection is the dorsal superficial lamina.

Figure 80-1. Dorsal hand arterial supply.

Figure 80-2. Sensory innervation of the hand.
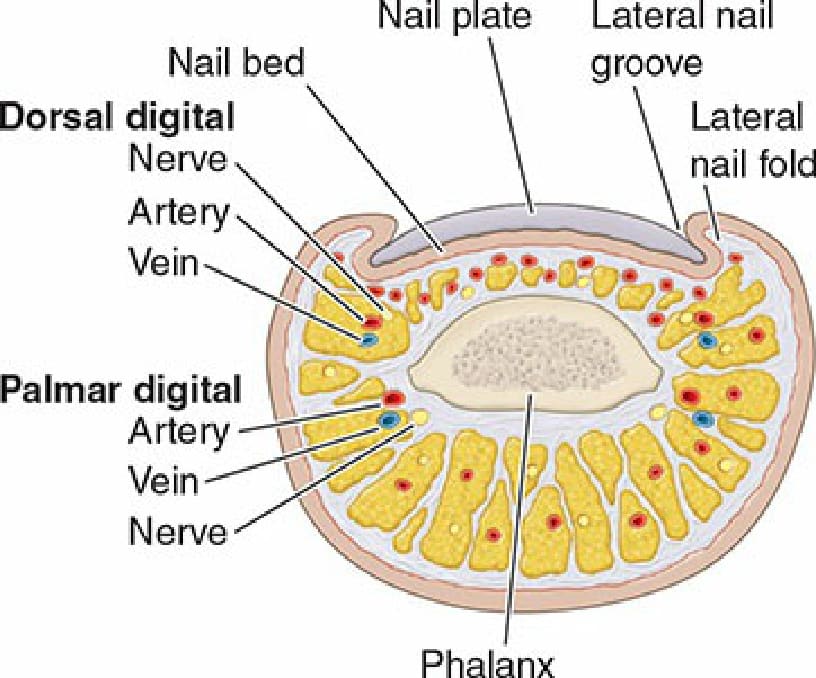
Figure 80-3. Cross-sectional anatomy of the digit.