Surgery
Surgery
Surgery for the neck consists of tightening and lifting lax skin and correcting platysmal bands. Surgery is still the gold standard for these two major elements of neck aging. A formal neck lift is essentially the posterior aspect of a lower facelift. The results are predictable and reproducible. It can be performed in the office setting with tumescent anesthesia. In most patients, this excisional surgery is combined with liposuction.
Platysmaplasty In many patients, the platysmaplasty is performed in conjunction with the neck lift. However, in a subset of patients who do not have lax neck skin, it can be performed as a standalone procedure. Its purpose is to correct the platysmal bands, and recreate the flat shield-like structure of this superficial muscle. Over the decades, there have been different methods to revise the bands. Unfortunately, there does not appear to be method that consistently, completely, and permanently smoothes these cords. The corset platysmaplasty described by Feldman involves suturing the two bands together inferiorly, and then superiorly in two rows.42 This is the classic method, but can be time consuming and increases the risk of bleeding and bruising. Other surgeons have recommended only lateral plication of the platysma, which will stretch the platysma and flatten the midline bands. However, this truly does not address platysmal hypertrophy. Other surgeons have recommended a transverse myotomy, though this may lead to stump formation and asymmetry. The method that one of the authors (HBG) utilizes is to approximate the platysma in the midline with four interrupted prolene sutures with lateral plication sutures.
More elaborate minimally invasive suture-based solutions for the platysma have been reported. Giampapa described an effective interlocking suture suspension lift for both the platysma and lax skin that demonstrated some effectiveness 13 years following the procedure.43,44 More recently, Mueller has created a percutaneous “trampoline” platysmaplasty and reported on his experience with 105 patients who maintained satisfactory results with a 33-month follow up.45 An accompanying cadaver study confirmed the tensile strength of the sutures. In addition to correcting platysmal banding, ptotic submandibular glands contribute to blunting of the cervicomental angle and a youthful neck. A suture sling suspension using either goretex or prolene can support the submandibular glands and the superior portion of a ptotic platysma. Small incisions on the neck posterior to the earlobe are made. The suture is then secured and fed through a 16-gauge liposuction cannula through the midline and to the other superior neck incision and secured. Multiple sutures create a hammock effect. The benefit of using goretex sutures is that they have a greater width than prolene, and theoretically could be tightened over time through small surgical procedures.
Surgical neck lift The surgical neck lift as mentioned above can be combined with neck liposuction and platysmaplasty depending on the aging characteristics of the patient’s neck. Essentially, a neck lift is a lower facelift without the anterior aspect. The goal of the neck lift is to significantly improve the contour of the neck, including the submentum, by lifting and tightening. This procedure can be performed with tumescent anesthesia and oral sedation. The incision starts at the anterior portion of the ear lobule, continues
posterior-superior along the postauricular sulcus to the height of the external auditory canal, and then courses posteriorly 5 to 6 cm into the scalp. The flap is undermined using a combination of Mayo, Gorny, and Baby Metzenbaum Scissors. If liposuction has been performed submentally, then it is also performed laterally where the flap has been incised. The neck is completely undermined below the subcutaneous layer. With severe actinically damaged skin, a fair amount of force may be needed given internal fibrosis, but care must be taken not to buttonhole this thin skin. When undermining the skin, scissor tips should be up, and care should be taken on the lateral neck where the external jugular vein is susceptible. The undermining needs to be particularly superficial near the great auricular nerve, along the mandible, and near the submandibular gland (Fig. 79-4).
Plication sutures can be absorbable or nonabsorbable, or a combination. Plication should be in a vertical direction. Borrowing from Knize, one author (HBG) will perform two sets of plication sutures: one set posterior, one set more anterior in order to maximize and maintain lift. The excess skin is then trimmed, allowing for minimal tension. The edges are sutured in two layers, and in most cases, a posterior dog ear will have to be removed. As with the other neck procedures, a compression garment is worn in the postoperative period.
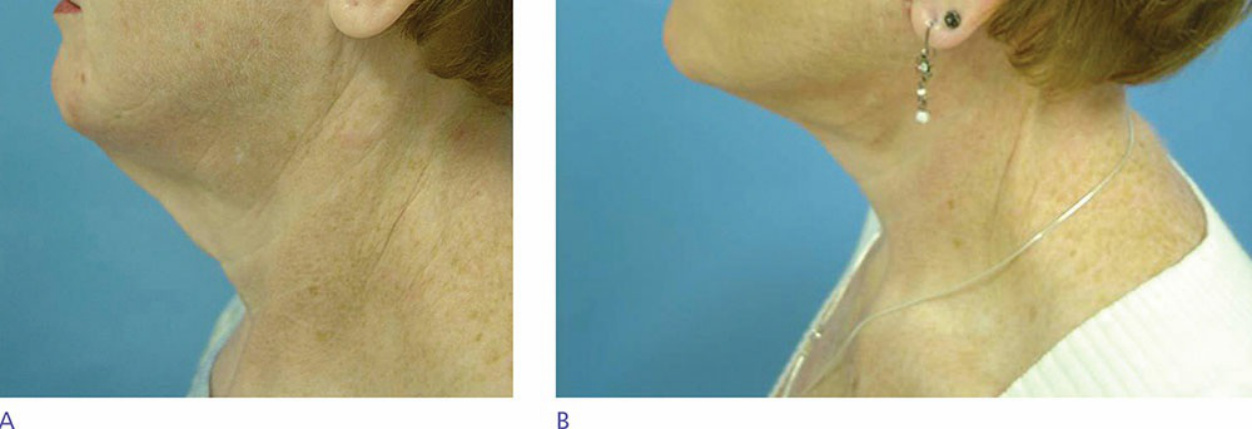
Figure 79-4. Surgical neck lift. (A) Before. (B) Three months postprocedure.