Acne
Acne
Medical management remains the first-line treatment for active acne, though chemical peels can be used as adjuvant therapy. Treatment of acne can be divided into therapies for active acne lesions and those for acne scars. Treatment and application regimens may differ between practitioners and are often not documented in detail in published case series, making extrapolation of results difficult. However, the superficial peeling
agents (salicylic acid, Jessner’s, glycolic acid, and low-concentration TCA) have all demonstrated efficacy in treating active acne lesions.
Salicylic acid peels, in particular, with their lipophilic and keratolytic properties, ease of application, and excellent safety profile, are commonly used. In a randomized single-blind prospective study comparing 30% salicylic acid peel versus Jessner’s solution applied every 2 weeks for 12 weeks in patients with mild and moderate acne, salicylic acid was significantly more effective at reducing comedone count (53.4% vs. 26.3%, P = 0.001).29 For papules, the overall difference at the end of 12 weeks was not statistically significant, though the group treated with salicylic acid peels saw improvement earlier.29 Patients from both groups experienced erythema and postinflammatory hyperpigmentation, but this was more frequent in the group treated with Jessner’s solution. This study was corroborated by a separate group that found that 30% salicylic acid improved both comedonal and inflammatory acne and showed greater efficacy versus Jessner’s solution for comedonal lesions.30 In this second study, no change in inflammatory lesions was seen with Jessner’s solution, but these results were only assessed after three peels, in contrast to six peels in the previous study.30 In another prospective, double-blind, randomized split-face study comparing 30% salicylic acid versus 25% TCA in patients with Fitzpatrick skin types III to V, both treatments improved comedonal and inflammatory lesions with no statistical difference between the two group. The authors noted no complications on the hemifaces treated with salicylic acid but did note prolonged erythema (25%) and hyperpigmentation (20%) in the group treated with TCA.31
Glycolic acid has also been found to be efficacious in the treatment of inflammatory and noninflammatory acne lesions. In one study using 70% glycolic acid applied for 2 to 8 minutes on the skin and repeated every 10 days as needed, the authors observed improvement with all stages of acne lesions, with comedonal acne improving the fastest followed by papulopustular acne and then nodulocystic lesions (average 3 treatments, 6 treatments, and 8–10 treatments, respectively). While nodulocystic lesions required more treatment sessions, the authors noted an additional benefit of improvement in superficial acne scars.32 In a separate prospective single-blind split-face study comparing 70% glycolic acid applied for 2 minutes versus Jessner’s solution, the authors saw improvement in both arms with no clear superiority for either treatment.33,34 Glycolic acid has also been compared to salicylic acid in a head-to-head prospective randomized, double-blind split-face study of mild to moderately severe acne. In this study, 30% glycolic acid was applied to one hemiface for 4 to 5 minutes while 30% salicylic acid was applied for 4 to 5 minutes to the other side. Both treatments decreased the number of acne lesions without clear superiority at 1-month follow-up. At 2-month follow-up, however, the side treated with salicylic acid had sustained this improvement while the side treated with glycolic acid demonstrated a trend toward
more new lesions.
Acne scars are another common condition that have been studied by the chemical peel community. In 2002, the chemical reconstruction of skin scars (CROSS) technique was introduced.35 A solution of high concentrations TCA (65% and 100%) is applied focally into the base of depressed acne scars using a sharpened wooden applicator to induce collagen regeneration (Figs. 78-4 and 78-5). Because the solution is focally applied, local anesthesia and sedation are not needed, and healing is faster than with traditional full-face peels. In the original 2002 case series, two blinded physicians evaluated pretreatment photos against those taken 6 months after treatment, and 15/15 patients receiving 6 or more treatment courses were deemed to have a good or excellent results (>50% improvement). In the group treated with 100% TCA, all patients receiving five or six courses showed excellent results (>70% improvement).35 In this Asian population, both groups experienced equal frequency of posttreatment erythema and transient postinflammatory hyperpigmentation. Studies involving the CROSS technique using 70% TCA, 90% TCA, and 88% phenol have all been reported and demonstrated efficacy for ice-pick scars.36,37 In a split-face trial of 90% TCA versus 88% phenol, both sides showed significant improvement in scar grades pre- and posttreatment, but patients rated phenol as more painful (5.3 vs. 4.4) on a 10-point pain scale. Persistent erythema and hyperpigmentation were seen in both treatment sides, but hypopigmentation and widening of scars were seen only in the 90% TCA group (two patients each, 14.3%).36 A similar case report of widening and atrophy of a scar was reported in a patient treated with an 80% TCA CROSS technique, suggesting that care must be taken in the application technique to limit the solution only to the scar depth.38
Actinic keratoses Chemical peels are an excellent modality for the treatment of diffuse actinic keratoses. In a head-to-head nonrandomized split-face trial, patients were treated with a single application of Jessner’s/35% TCA medium depth peel on the left side of the face and a traditional 3-week regimen of topical 5-fluorouracil on the right side of the face and then evaluated at 1, 6, and 12 months. Both sides received pretreatment with tretinoin 0.025% cream nightly for 2 weeks. Both hemifaces showed a significant reduction in the number of actinic keratoses (75%), with neither showing superiority at any follow-up endpoint.39 This was confirmed histologically by biopsies taken at the 1-month followup, which showed significant reduction in hyperkeratosis and parakeratosis compared to pretreatment biopsies. In a questionnaire completed at the 6-month visit, all but one of the respondents reported preference for the chemical peel due to the convenience of a single treatment and the shorter healing time.39
In contrast to medium depth peels, superficial peels alone are often inadequate in the treatment of actinic keratoses. In a prospective, randomized, controlled split-face study evaluating weekly application of glycolic acid alone versus glycolic acid with 5- fluorouracil over 8 weeks, the sides treated with the combination (fluohydroxy pulse
peel) demonstrated a 92% (range 81–100%) reduction in AK compared to only 20% in the monotherapy group (P < 0.05).40 Both investigators and patients reported preference for the side treated with the combination therapy. In addition to the reduction in actinic damage, there was also improvement in the overall cosmesis with reduction of solar lentigines, telangiectasias, and rhytides.
Melasma Melasma is an acquired hyperpigmentation disorder that is challenging to treat. Medical therapy remains first-line and consists of sun protection with some combination of hydroquinone, tretinoin, and a topical steroid, but patients often show variable results and recurrence is high. Chemical peels can be used as an adjunct therapy and numerous variations in treatment regimen have been reported in the literature. In general, serial treatments are needed to prevent relapse, combination treatments are better than monotherapies, and postinflammatory hyperpigmentation remains a risk factor.
Melasma is commonly divided into epidermal, dermal, and mixed types with the aid of a Wood’s lamp. Most studies use superficial peeling agents to target the epidermal and dermal pigmentation and deeper peels to target mixed pigmentation. In a split-face trial comparing Jessner’s solution versus 70% glycolic acid applied for 2 minutes applied 1 month apart over 3 months, both sides achieved improvement with an average MASI score decrease of 8.61, with no superiority in either arm.41 While this decrease is on par with what has been reported with medical therapy alone, the improvement occurred over 3 months as opposed to 10 months. Interestingly, however, Wood’s lamp illumination to determine the depth of pigment was not useful in predicting clinical response. Another study investigating the effect of 55% to 70% glycolic acid and 10% to 15% TCA in 100 patients showed that half of the patients required fewer than 5 peels while half required 5 to 10 peels. While the patients treated with TCA required fewer number of peels (4.1 vs. 6.1), this group also experienced higher rates of relapse and hyperpigmentation (25% vs. 5.9%).42 Of note, no discussion was made of a priming regimen.
Multiple studies have shown that a combination approach using a topical regimen with serial chemical peels can improve melasma. In two independent studies, when patients were primed with hydroquinone 2% or tretinoin 0.025% cream nightly for 2 weeks prior to a series of six peels (10% TCA in one study, 20%+ glycolic acid in the second), both groups showed an initial improvement that was comparable, but the group treated with hydroquinone experienced longer duration of their effect with less relapse.26,27 In another study evaluating the additional benefit of serial glycolic acid peels, patients were randomized to either medical therapy alone (topical azelaic acid 20% cream and adapalene 0.1% gel) or medical therapy with a series of eight glycolic acid peels (35–70%). The combination treatment group achieved an 83% decrease in
mean MASI score, compared to 69% in the medical treatment group.43
Other peels have also been studied in the use of melasma. The data on serial salicylic acid are mixed, with one study reporting efficacy and another finding no improvement. A randomized, single-blind study divided 60 patients with epidermal melasma into two groups treated with either Jessner’s solution (34) or 30% salicylic acid (26). Patients were primed with 0.05% tretinoin cream for 2 weeks and counseled to use SPF 60 sunscreen and then treated biweekly over 12 weeks (six treatments) with their respective chemical agents. Both groups saw statistically significant improvement, as measured by their MASI score at the end of the treatment period and at the 4- and 12- week follow-up visits.44 No superiority in either arm was detected. A more recent prospective, randomized, controlled, split-face trial of epidermal melasma compared a series of four salicylic acid peels applied biweekly in conjunction with 4% hydroquinone cream versus hydroquinone cream monotherapy. While both treatment regimens showed improvement by the treatment end, no superiority was seen with the addition of salicylic acid peels.45
Melasma is a difficult condition to treat. It is difficult to conceptualize the mechanism for superficial peels to improve dermal melisma. It may be that the majority of melasma is mixed and the improvement seen in dermal melisma is that of the epidermal component. To offer patients the best chance of success, patients should be primed and maintained on a topical regimen which includes hydroquinone with an expectation that serial peels will be needed to achieve improvement, but relapse will likely recur.
Facial rejuvenation Facial rejuvenation and improvement of photoaging is one of the primary applications for chemical peels. To guide clinicians in the assessment of photodamage, the Glogau classification can be used in assessing the patient (Table 78-8). Superficial peels can improve skin texture and mild hyperpigmentation while medium depth peels target more extensive actinic damage and fine lines. For deeper etched-in lines, however, deep peels should be used. Glycolic acid is one of the most popular superficial peels for facial rejuvenation. Patients can be given a pre-peel regimen of tretinoin and/or low concentration glycolic acid cream and then peeled with serial glycolic acid treatments with increasing concentration (50–70%) as their skin tolerance allows. For the treatment of wrinkles and solar lentigines, 70% glycolic acid may be left on for 4 to 8 minutes.46 The beneficial effects of glycolic acid have also been tested and confirmed in a prospective placebo-controlled split-patient study evaluating a 50% glycolic acid gel formulation applied for 5 minutes on the face, forearm, and hands compared to a vehicle control. After 4 consecutive weekly treatments, patients were evaluated by blinded evaluators both clinically and by biopsy. Across the three site locations, glycolic acid

Figure 78-4. CROSS technique: Frosting immediately upon application (A, B); early postop erythema (C, D).
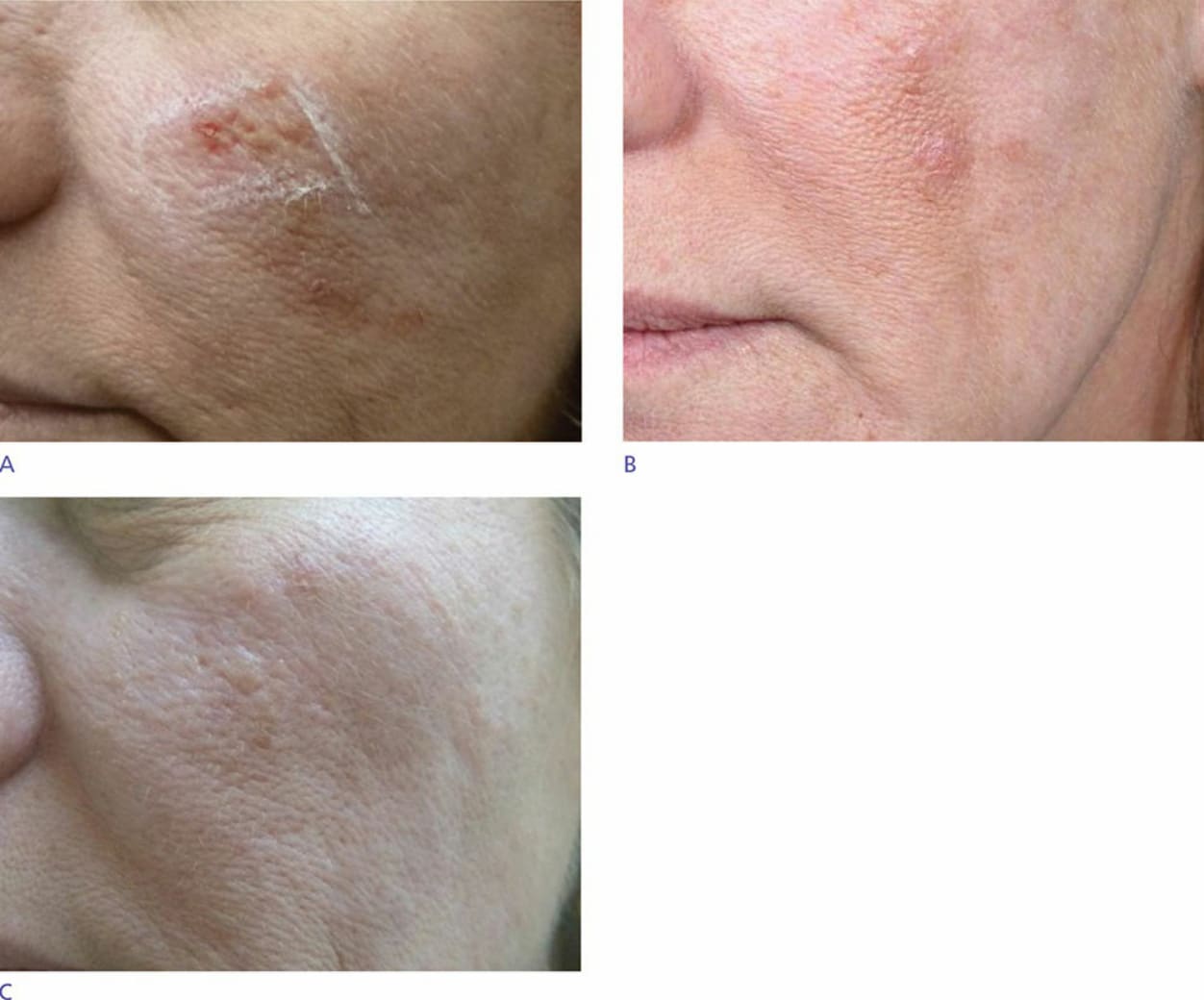
Figure 78-5. CROSS technique: Pretreatment (A); 3 months posttreatment (B); 2 years postop (C).
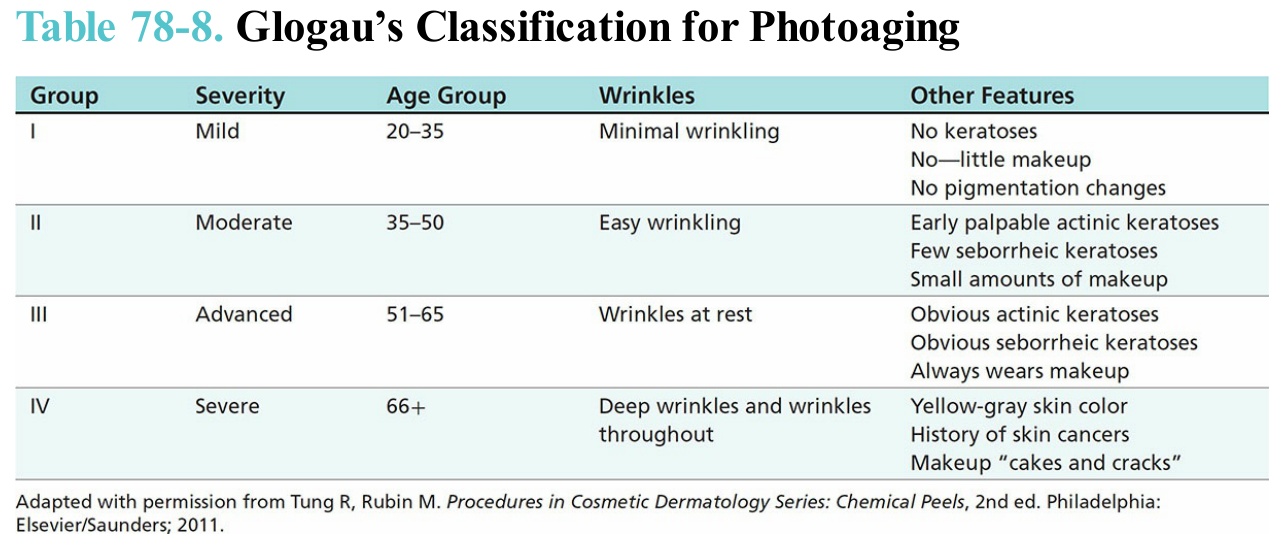
Table 78-8. Glogau’s Classification for Photoaging