Skin characteristics
Skin characteristics
When assessing the patient for a chemical peel, the first and foremost consideration should be the patient’s skin type and characteristics. Even with the same application technique, differences between patients can significantly alter the penetration of chemical peels and affect their safety and efficacy. In selecting the appropriate peel, the dermatologic surgeon must first consider the patient’s tendency for postinflammatory hyperpigmentation. Patients with Fitzpatrick’s skin types IV to VI (Table 78-4) have a greater risk of postinflammatory dyschromia. While superficial peels carry less risk for adverse events such as hyperpigmentation, hypopigmentation, or scarring, patients should still be given an appropriate pre-peel regimen and practice sun protection postpeel.2 Test spots in less cosmetically sensitive locations can also be performed prior to a full procedure. In addition to patients’ natural tendencies toward pigmentation, inherent skin texture can also affect the efficacy of the peel (Table 78-5). Areas of active inflammation allow deeper penetration of chemical solutions compared to surrounding skin, leading to deeper ablation. Patients with rosacea, in particular, may experience greater inflammation and are at greater risk of prolonged erythema post-
peel. Patients with thin and translucent skin will similarly experience greater ablation with greater risk for adverse events. In contrast, patients with thick sebaceous skin or those with hyperkeratotic lesions will experience less penetration and must be prepped appropriately to elicit the intended reaction. Similarly, with the same peeling regimen, areas of the face with thinner skin will experience greater penetration compared to areas of thicker skin.5
Medical and surgical history When taking a medical history, the physician should probe for any risk factors associated with poor healing and poor outcomes (Table 78-6). Patients with a history of hypertrophic scars or keloid formation should be limited to very light superficial peels
to avoid dermal damage. Those with an active herpes simplex virus infection should wait until active sores are healed and then treated prophylactically prior to their procedure to avoid triggering another outbreak and dissemination of the virus on resurfaced skin. If a history of HIV or nicotine use is elicited, the patient should be counseled regarding the potential for delayed wound healing. Patients with recent isotretinoin use should also be counseled regarding the risk for delayed healing and abnormal scarring, even with superficial peels. While there have been case series questioning the need to delay peels for 6 or 12 months after completion of isotretinoin therapy, there are case reports of scarring and prolonged hyperpigmentation and erythema in patients with recent low-dose isotretinoin use, even when treated with superficial peels.23,24 In one such case, the patient had previously tolerated 70% glycolic acid while on isotretinoin without any adverse events, suggesting that reactions may be unpredictable and idiosyncratic.23
When eliciting surgical history, the physician should probe for any history of radiation or prior facelift or browlift. Radiation decreases the vasculature and density of pilosebaceous units from which the skin regenerates, thereby delaying healing.
Similarly, if the patient has had prior facial surgery with extensive undermining, the superficial plexus may be disrupted in the immediate postoperative period, delaying healing. Finally, female patients of child-bearing age should also be questioned about any possibility of being pregnant or if they are breastfeeding.
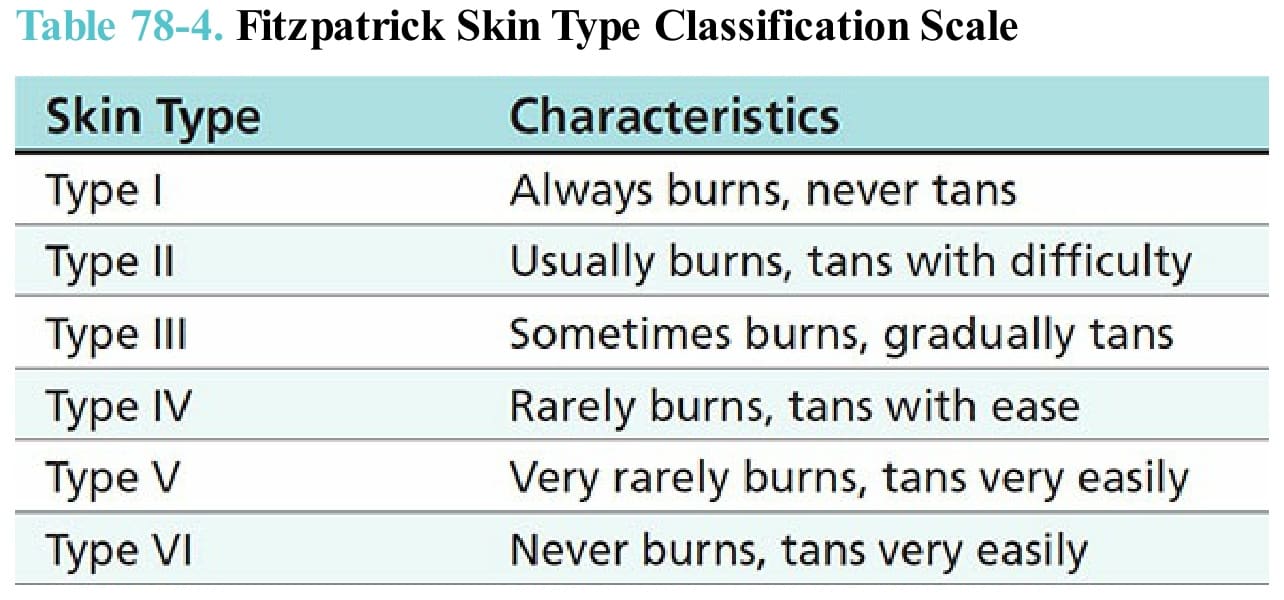
Table 78-4. Fitzpatrick Skin Type Classification Scale
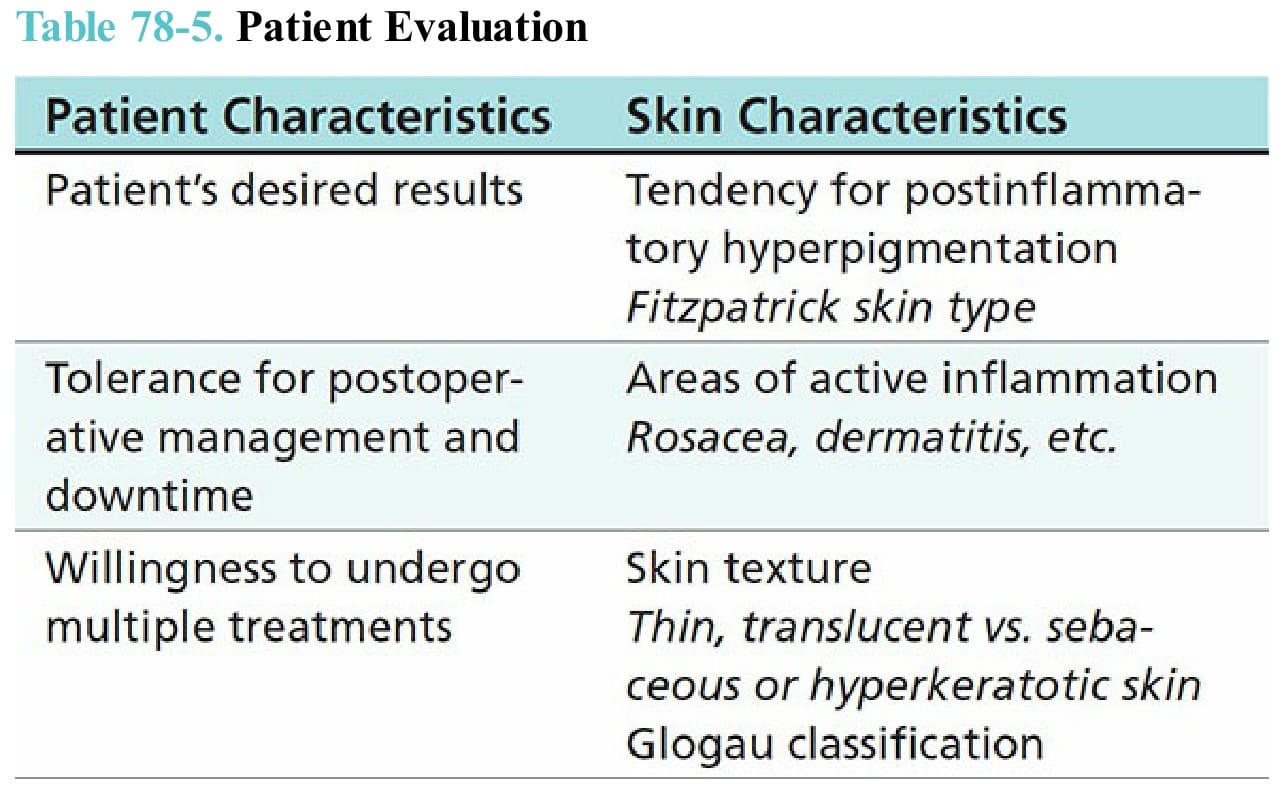
Table 78-5. Patient Evaluation
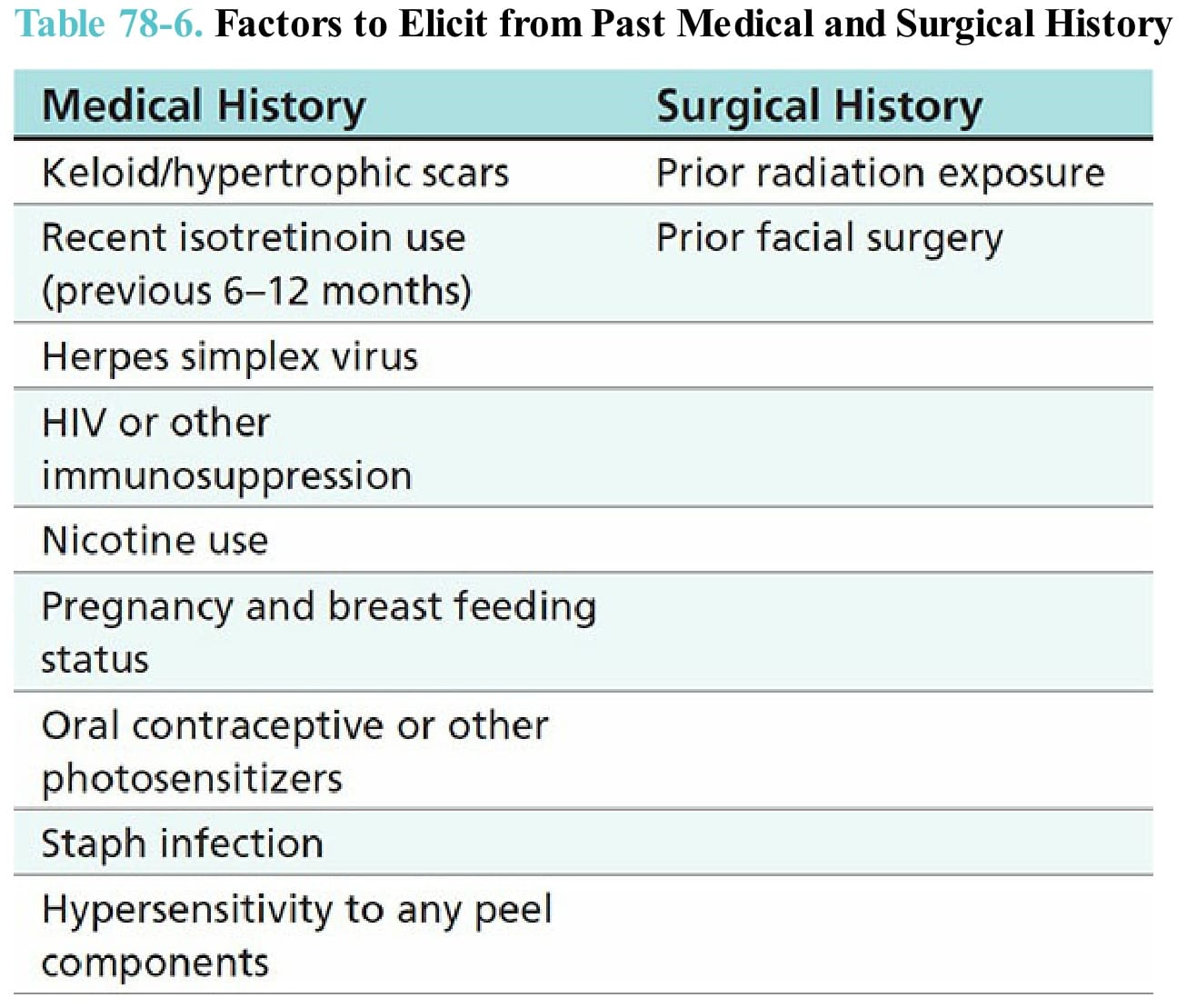
Table 78-6. Factors to Elicit from Past Medical and Surgical History