Phenol-based solution
Phenol-based solution
Phenol-based peels provide the deepest chemical ablations and can be used for etchedin wrinkles resistant to all other peels. The most common formulation used is the Baker–Gordon phenol solution (Table 78-3).14 This formulation should be freshly prepared and frequently stirred to ensure an exact and even concentration is applied. There have been many modifications to this original formulation, including the Exoderm and Venner-Kellson solutions, which are better tolerated with an improved safety profile and less penetration.15,16 As with the previously discussed peels, penetration is not solely determined by the formulation. While increasing concentrations of phenol and croton oil lead to greater tissue damage, the application technique itself is important; more vigorous application with greater coats leads to a deeper peel and more inflammation.17–19
Patient selection is critical given the discomfort, extensive healing process, and potential for adverse events associated with phenol peels. Patients are commonly put under sedation for their comfort, as the process can otherwise be painful. Patients should also have cardiac monitoring and intravenous hydration throughout the procedure to minimize the risk of cardiotoxicity. The patient’s face is first cleansed and degreased with acetone. This is followed by application of a thin layer of freshly mixed Baker’s formula using cotton-tipped applicators, taking care to avoid excess solution. This is applied first to the forehead, then the cheeks and perioral and nasal skin. The entire procedure should be performed slowly over 60 to 90 minutes to slow the systemic absorption of phenol and decrease the risk of cardiotoxicity. The skin will immediately frost due to protein coagulation as each site is treated. To delay the absorption, the clinician should wait 15 minutes between each cosmetic unit. Each zone should be feathered out into the surrounding skin to avoid sharp demarcation between treated and untreated regions. Patients should have cardiac monitoring throughout the procedure and for 1 hour postoperatively. Once completed, the peel can either be left open or placed under occlusion with waterproof zinc oxide tape. If left open, patients should be counseled to expect erythema and edema and to apply petrolatum ointment liberally twice daily. Unoccluded phenol peels have penetration similar to medium depth peels, so patients should expect faster healing times. For deeply etched wrinkles, patients will need a phenol peel occluded by waterproof zinc oxide tape placed in overlapping strips over the entire treated surface. This should be left on for 24 to 48 hours. At the return visit any drainage or excess exudate can be gently removed. A second mask formed from bismuth subgallate powder can then be applied with reapplication of the powder at home as needed for the next week. By the end of the week the skin will have reepithelialized and this second mask is removed with petrolatum ointment and warm compresses.7,16
When performing deep peels, the clinicians should be aware of potential complications. In a study of 43 consecutive patients undergoing phenol-based peels, half of the patients who had their peels completed within 30 minutes developed cardiac arrhythmias compared to none of the patients who had their peel completed over at least 60 minutes.20 The arrhythmias included premature ventricular contraction (4), bigeminy (2), paroxysmal atrial tachycardia (2), and ventricular tachycardia (2), with no
correlation with age (range 24- to 73-year-olds). In the 10 patients who developed arrhythmias, 9 had unremarkable preoperative EKGs.20 The incidence of cardiac arrhythmias can be reduced when precautions such as intravenous hydration, proper ventilation, and prophylactic propranolol are given. In a retrospective case series of 181 patients treated with a full-face Exoderm phenol peel, which slows the absorption of phenol compared to the traditional Baker–Gordon formula, 6.6% of patients still developed an arrhythmia when the treatment was completed over 30 minutes despite concurrent treatment with intravenous hydration, 1 mg of prophylactic propranolol, and an electric fan and air conditioned room to improve ventilation.21
Aside from cardiac complications, phenol peels are also susceptible to hyperpigmentation, hypopigmentation, prolonged erythema, and scarring. Even though the Exoderm modified phenol peel decreases the risk of adverse events, a case series involving Asian patients still showed frequent side effects including postinflammatory hyperpigmentation (74%) and prolonged erythema of more than 3 months (11%).22 Hypopigmentation was rare, but did occur in 1 of 46 patients (2%).
Similar to TCA solutions, phenol can also be applied as monotherapy at high concentration in the treatment of depressed acne scars. Because the application area is limited, this targeted treatment method has low absorption and an improved risk profile, but patients should still be counseled on the risk of dyschromias and erythema.
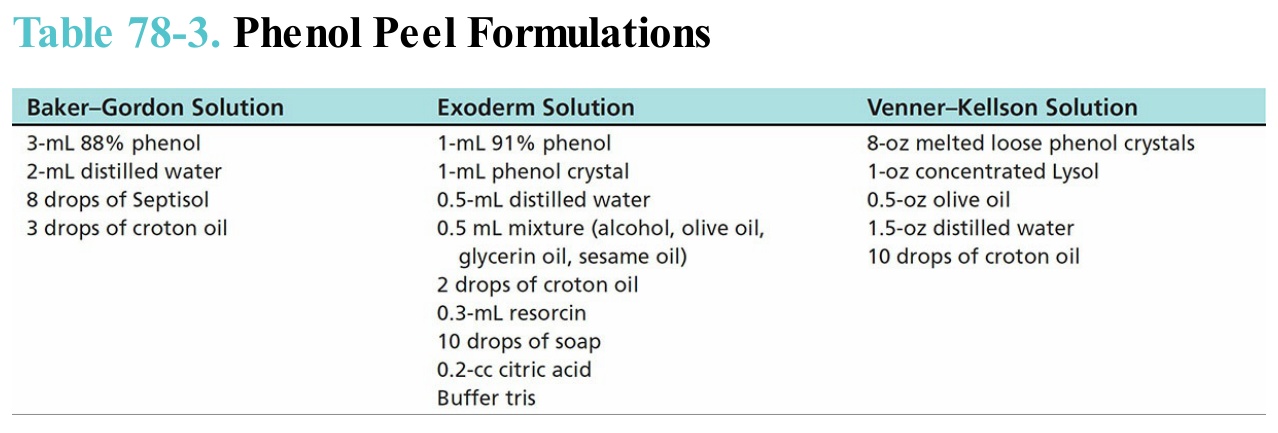
Table 78-3. Phenol Peel Formulations