Telangiectasias
Telangiectasias
For a patient presenting with nasal or facial telangiectasias, the long-pulsed PDL, Vbeam Perfecta, KTP/Nd:YAG, or IPL may be used (Fig. 77-8). For telangiectasias of
the neck or chest, the larger spot-sized IPL devices allow more efficient treatment, with appropriate judicious adjustment of fluence.
- Most laser devices for treatment of vascular lesions are based on a fiber delivery
system with a contact or dynamic cooling device. For contact cooling devices, a water-based gel is placed directly on the skin, and the crystal or spacing device is held directly against the skin. In contrast, for dynamic cooling, no gel should be used because the cryogen cools the skin. Gel is not necessary with PDL, and may introduce water that diminishes the fluence before reaching the target vessels. Minimal pressure is placed against the skin, as the target may be compressed with excessive hand pressure. Treatment parameters are outlined in Tables 77-4 and 77-5. See also for utilizing both KTP and PDL for treatment of nasal telangiectasias.
- If using an IPL device, use the filter with cutoffs at 560 to 590 nm. Rarely, the 515-nm
cutoff filter can be used in patients with type I or II skin. For devices that have fixed filters, use an IPL head that produces green or yellow wavelengths. If a contact cooling device is utilized, a small layer of water-based or coupling gel is placed on the skin. With minimal pressure, the cooling device with crystal is placed directly onto the skin overlying the targeted area. No pressure is applied, as the target vessels collapse with compression leaving very little target. Figure 77-9 shows placement of the IPL crystal with gel on the skin. An immediate gray tone to the skin in the shape of the crystal is not desirable; pronounced erythema and urtication in the shape of the crystal should be avoided as well. The Cynosure ICON MaxG for the face and MaxY for the neck and chest may be used at 10 to 20 ms and 25 to 42 J/cm2 and the Lumenis One at 3 ms, double pulse, with 10 to 20 ms off time between pulses at total fluence of 14 to 20 J/cm2. The ICON has the added advantage of the SkinTel, which determines the patient’s melanin index and suggests a range of safe treatment parameters based upon that. Extended pulse durations may be used for larger nasal telangiectasias with pulse durations of 40 to 50 ms (Figs. 77-10 and 77-11). Pulse stacking can be done on the face, nose, neck, and chest, and enhances efficacy. During a lengthy treatment, some device crystals may start to warm up; one must be alert for this. Treatment parameters are outlined in Table 77-6 and demonstrated in.
- Regardless of the light source or laser utilized, there are some features and pitfalls
common to all devices. Typical endpoints include immediate vessel contraction, visible intravascular photodarkening, which represents intravascular coagulation, or rupture of the vessel causing immediate purpura. In general, purpura may be avoided without compromise of efficacy, and purpura causes significant patient downtime. The pulse duration should be extended when purpura is encountered. If vessel constriction is not noted, either the energy needs to be increased or the pulse duration may need to be increased, as the entire vessel may not be heating. The risk of hyperor hypopigmentation from overcooling the skin with cryogen also exists. Blanching is to be avoided with all devices. For the PDL and KTP lasers and IPL, up to three passes may be performed over the treated area.
4. With the 1,064-nm lasers, the Cutera Excel V or CoolTouch Varia is commonly used;
there are multiple lasers available with similar wavelengths. For telangiectasias of the nose (not ala), face, neck, or chest a pulse duration of 30 ms, fluences of 110 to
120 J/cm2, spot size of 5 mm, and cooling at 5oC may be used. Lateral spread of thermal effects within the vessel beyond the point of treatment is frequently noted so that overlap is not necessary; pulses should be spaced out by at least 1 mm. Stacked pulsing, which can be performed with PDL and KTP, should never be utilized for infrared lasers, particularly 1,064-nm lasers. The 1,064-nm laser is especially effective at treating blue 1 to 3-mm telangiectasias of the forehead.
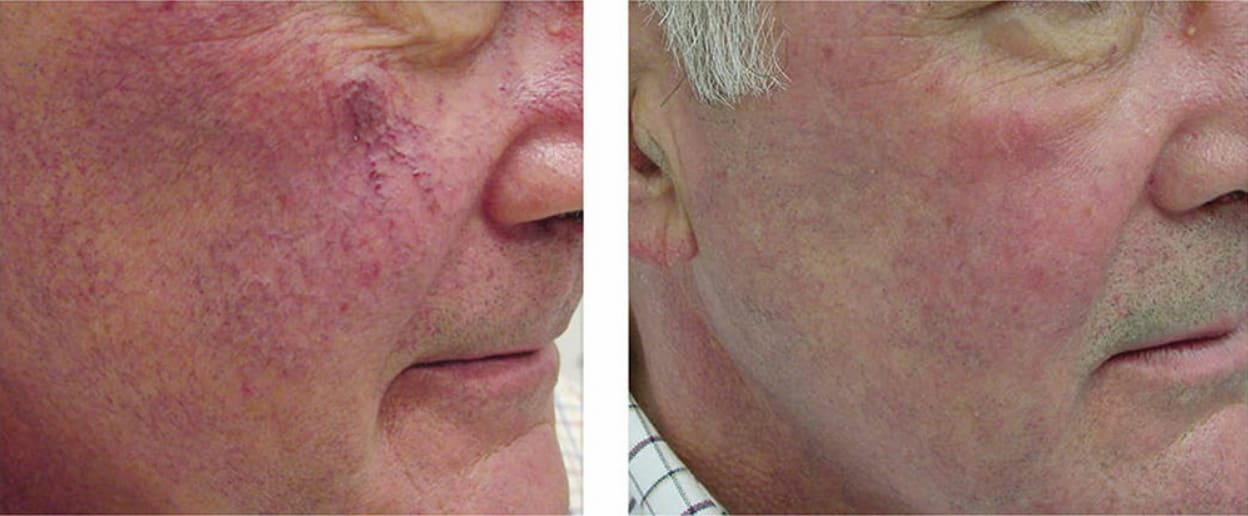
Figure 77-8. A 55-year-old male presented with worsening facial telangiectasia (left). Note the marked improvement after three treatments with both 1,064 nm for the larger telangiectasias and 532-nm treatment for the smaller telangiectasias (right).
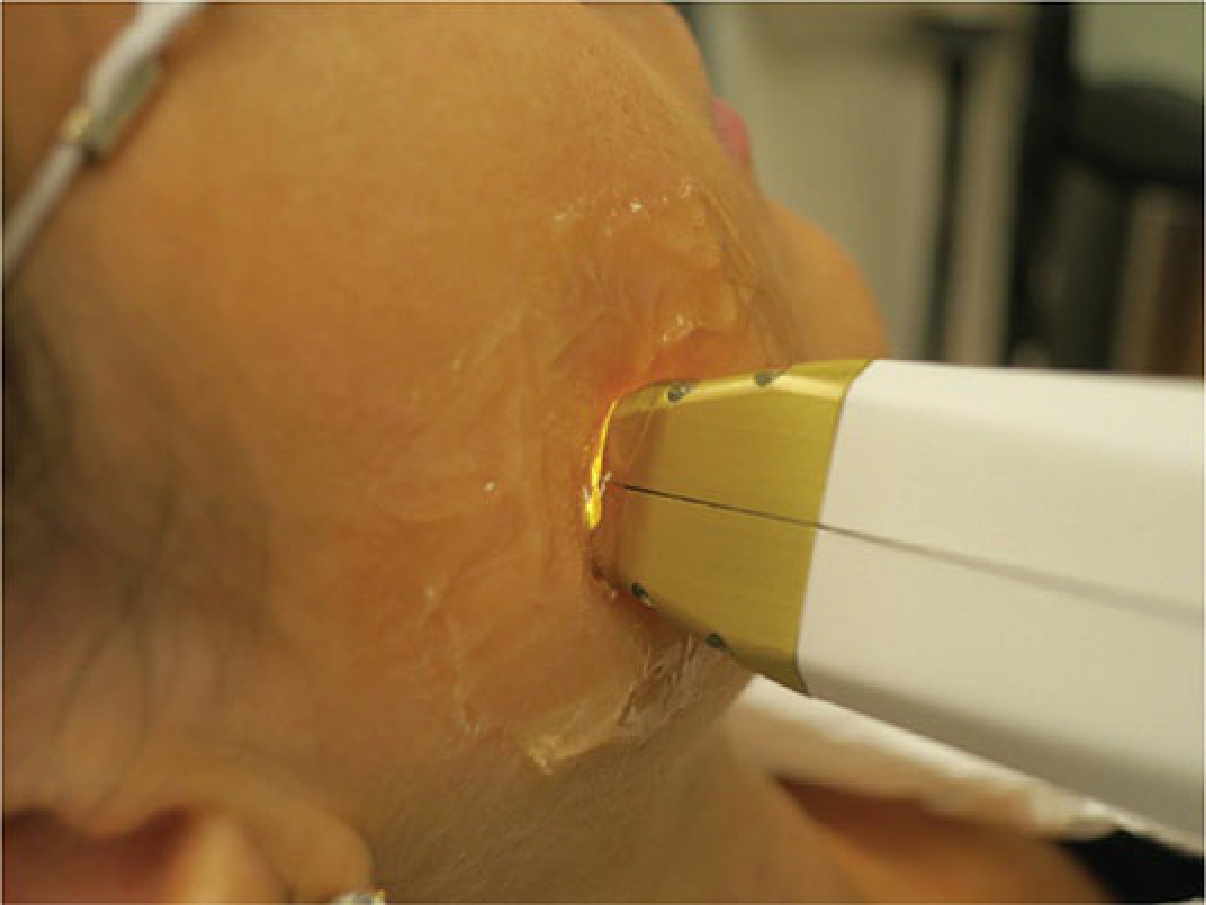
Figure 77-9. IPL device with cooling gel on the skin.
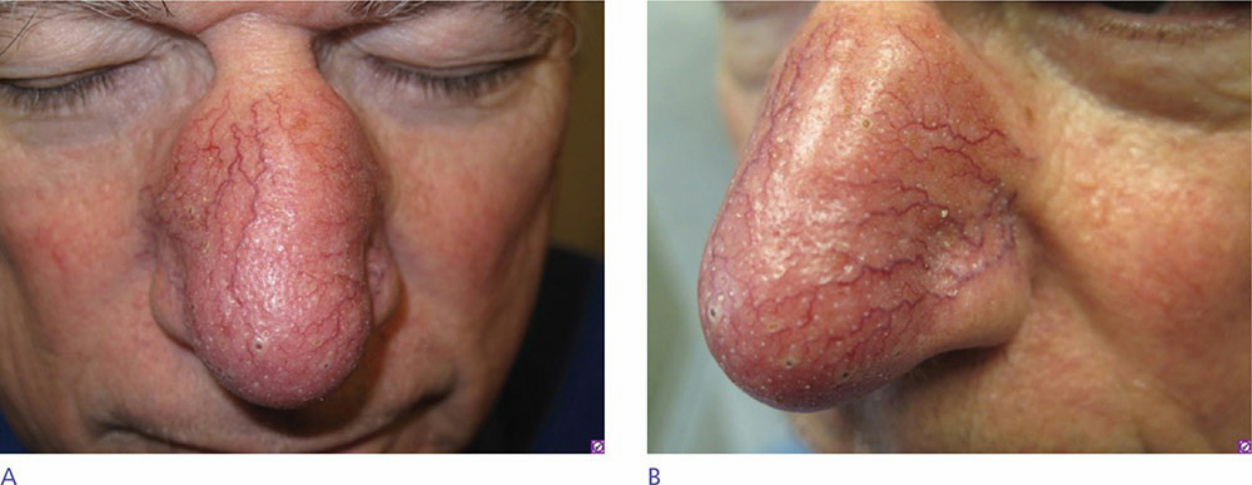
Figure 77-10. A 65-year-old male presented with rhinophymatous rosacea. He was treated with a combination of Vbeam Perfecta and Excel V (both KTP and Nd:YAG) given the combination of diffuse erythema and large discrete telangiectasias. Care was taken not to pulse stack with the Nd:YAG, whereas pulse stacking was utilized with the PDL.
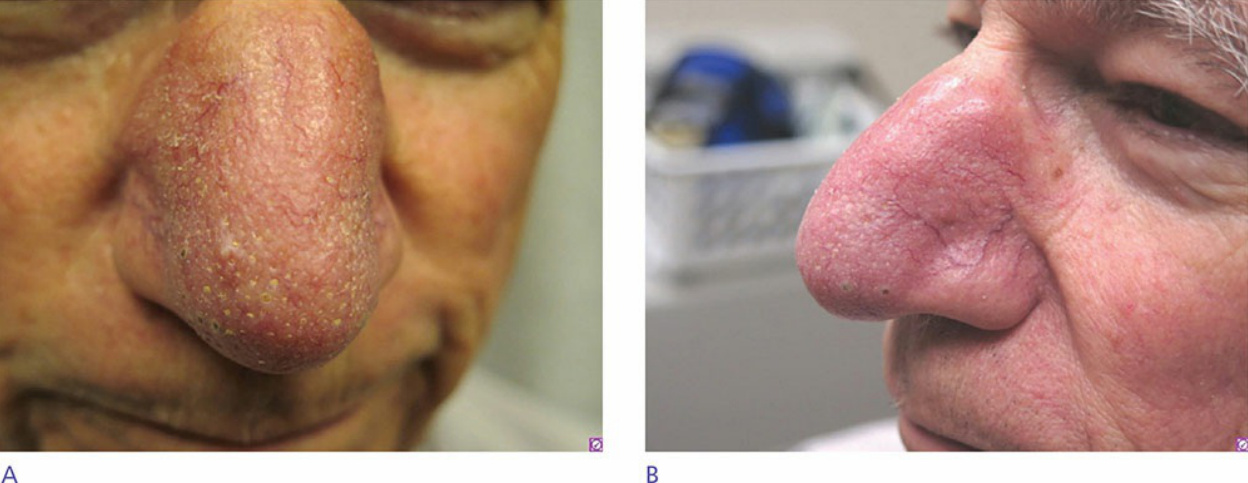
Figure 77-11. The same patient after a series of four treatments.
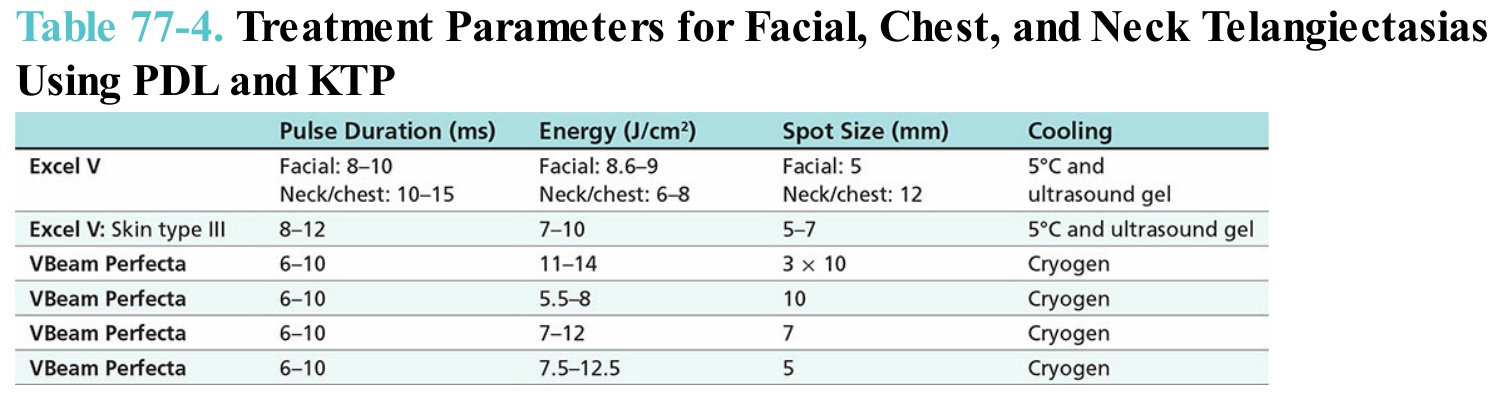
Table 77-4. Treatment Parameters for Facial, Chest, and Neck Telangiectasias Using PDL and KTP
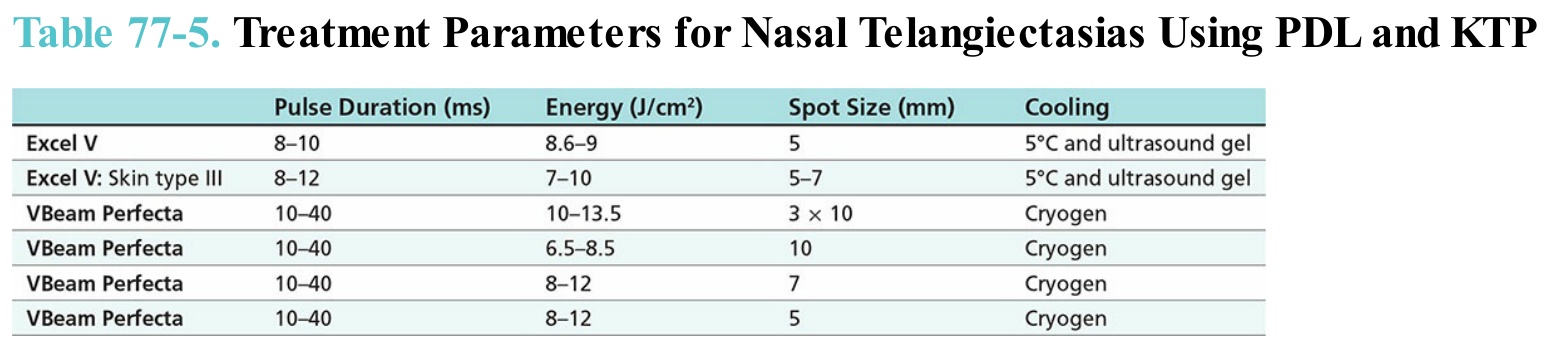
Table 77-5. Treatment Parameters for Nasal Telangiectasias Using PDL and KTP
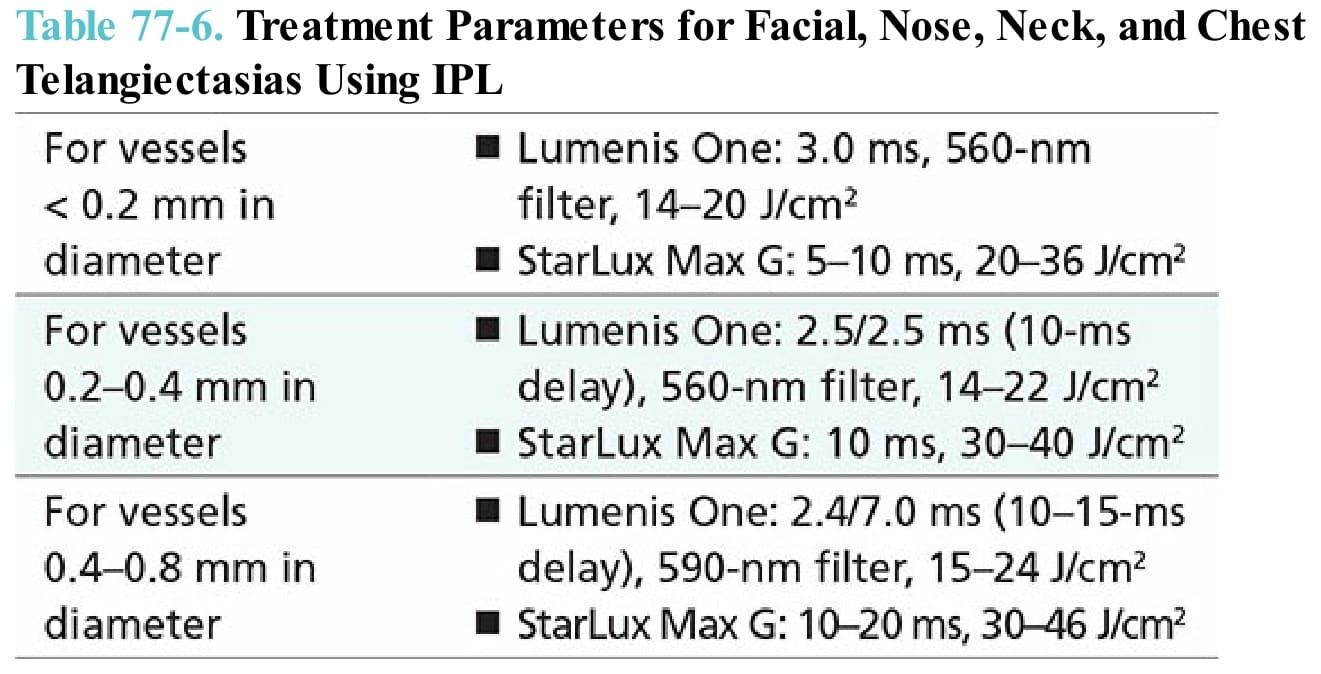
Table 77-6. Treatment Parameters for Facial, Nose, Neck, and Chest Telangiectasias Using IPL