Clinical manifestations
Clinical manifestations
PIH clinically presents as hyperpigmented macules in the same distribution as the initial trigger. The color of the lesion is determined by the location of the excess pigment, and the intensity of the pigmentation correlates with the higher skin phototypes. Further, PIH tends to worsen with UV exposure or with persistent or recurrent inflammation.
Other causes of dyschromias include a wide range of disorders like Riehl melanosis, lichen planus pigmentosus, erythema dyschromicum perstans, facial pigmentary demarcation lines, and Poikiloderma of Civatte. The etiology in most of these entities is unknown, but factors such as exposure to UV radiation, chemicals, allergens, and photodynamic substances in cosmetics have been implicated.8 Apart from these acquired dermatoses of dyspigmentation, certain disorders like Nevus of Ota are also well-known causes. A brief description of the etiology, clinical features, and the histopathology of some of the other important causes of dyspigmentation is detailed in Table 76-1.
MANAGEMENT
The management of dyschromia entails a multimodal approach addressing multiple factors contributing to the development of the disease. Many of these factors are not completely understood, adding an additional dimension of difficulty to the treatment of the various diseases. The therapeutic plan primarily consists of identification and removal of causative as well as triggering factors and stringent photoprotection coupled with the use of depigmenting agents. Apart from the aforementioned interventions, counseling forms an integral component of the management, whereby patients need to be informed about the natural history of disease, length of the treatment, and tendency to persist or recur. Furthermore, efforts should be made to understand the impact of the disease on the QOL of the patients and the treatment plan should also be aligned such as to provide maximum improvement. Additionally, use of cosmetic camouflage should be offered to patients during the treatment as well as an alternative for those who cannot use or tolerate therapy.
Sun avoidance is the most important part of the treatment of hypermelanoses, both for current improvement and future prevention of recurrence. Additionally, use of sunscreen has been documented to increase the efficacy of topical hydroquinone (HQ)-based treatments.9,10 Rigorous sun protective behavior should be instilled in the patients including the use of broad spectrum sunscreens (UVA and UVB) along with physical blocks (zinc oxide or titanium dioxide) with a minimum sun protection factor of 15, along with sun protective hats and clothing.
Pigment reduction can be brought about by both medical and physical modes of treatment. As there is no universally effective treatment and efficacy of existing agents is variable, responses can vary and relapses are frequent. The treatment options include multiple topical and oral depigmenting agents, chemical peels, and physical modalities such as dermabrasion and lasers. Among the medical treatments, HQ and triplecombination creams (HQ + retinoic acid [RA] + corticosteroid [CS]) remain the gold standard, while other options include dual combinations (HQ + RA, CS + RA, HQ + CS), kojic acid, azelaic acid, arbutin, ascorbic acid, tranexamic acid, mequinol, rucinol, lignin peroxidase, orchid extracts, licorice extract, and various other botanicals which are in different stages of development. Other treatment options include chemical peels like glycolic acid (GA), mandelic acid, lactic acid, Jessner’s and retinoid peels as well as lasers like Q-switched neodymium-doped yttrium aluminum garnet (QS Nd:YAG) laser (1,064, 532 nm), Q-switched ruby (694 nm), and Q-switched alexandrite (755 nm).
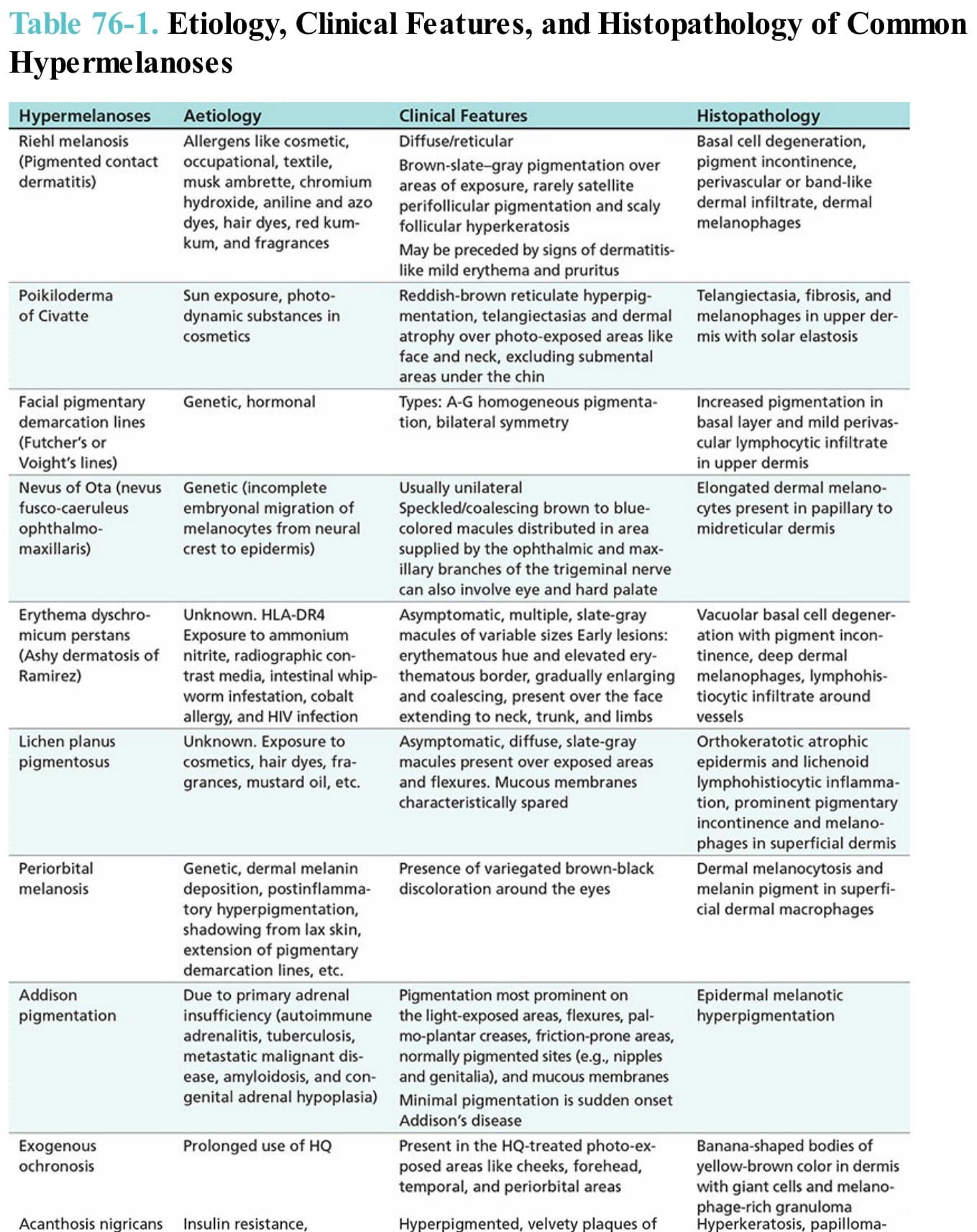
Table 76-1. Etiology, Clinical Features, and Histopathology of Common Hypermelanoses