Fillers
Fillers
Three injection planes have been suggested, and these can be combined to achieve the best aesthetic results in the lateral canthal area. These include a superficial plane positioned immediately above the orbicularis oculi muscle, a midlevel layer immediately below the orbicularis muscle, and a deep layer above the periosteum.48 Filler selection will depend on the injection plane. HA products with lower viscosity and minimal lift capacity are desirable for superficial and midlevel placement to minimize the risk of the Tyndall effect and visible product accumulation. Juvederm Volbella, Juvederm Ultra, Restylane Defyne, Restylane Fynesse, and Belotero Balance are a few examples. Deeper volumizing injections are best achieved with HA products such as Juvederm Volift, Juvederm Ultra Plus, Restylane Defyne, and Belotero Intense.27
Deeper injections may be achieved with linear threading or serial microaliquots using a blunt 27-gauge 1½-in cannula or sharp 30-gauge or smaller needle injections. The entry point for microcannulas can be located approximately 1 in below the lateral canthal commissure.29 The risk of intravascular injection into the medial zygomaticotemporal vein may be lessened by using blunt microcannulas.49 The lateral canthal tendon or lateral palpebral ligament is a fibrous structure attaching the lateral
canthus and integrating it into a dense connective-tissue structure (Whitnall’s tubercle) to bone. Stretching the lateral canthal tendon with deeper filler placement might lead to a taut lower eyelid with resultant globe overprojection.
Sharp needle microaliquots or cross-hatching injections may be desirable for more precise placement in the superficial and mid layers. Placement in both planes yields “sandwiching” of the orbicularis oculi muscle with resultant improvements in dynamic and static rhytides and skin texture.48 Midlevel plane injections should be targeted toward the lateral suborbicularis oculi fat pad.50
Botulinum toxin Botulinum toxin is the cornerstone of treatment of lateral canthal rhytides. Dynamic rhytides are primarily caused by contraction of the lateral portion of the orbicularis oculi muscle. Zygomaticus muscle activity may also contribute to inferior lateral canthal rhytides. Four patterns have been described for crow’s feet; full, upper, lower, and central fan (Fig. 75-11).51,52 The upper fan pattern was observed in only 10% of individuals studied.48
Onabotulinumtoxin A was FDA-approved for crow’s feet treatment in 2013.53,54 The global aesthetics consensus recommends an equivalent total of 6 to 25 units of intracutaneous onabotulinumtoxin A per side, with doses as low as 4 units in some cases. The number of injection points can vary between 1 and 5 per side. Injection of 1 to 4 units to the uppermost portion of the orbicularis oculi can also provide brow
elevation. Reducing the dose per injection site to the inferior lateral orbicularis oculi was recommended to minimize spread of neuromodulator to the zygomaticus muscle, thus reducing the risk of smile asymmetry and a shelf-like appearance when smiling. The consensus panelists also recommended avoiding a second row of injections for rhytides extending toward the temporal hairline; however, this can be done for severely sun-damaged skin, or in patients who have undergone cosmetic surgery, such as face lifting with consequent extension of rhytides as far as the hairline.33 In addition, the injector may want to inject oriented away from the eyes with needle bevel up and 1 cm lateral to the orbital rim to prevent diffusion of the product into the orbit.
Customized injection configurations according to the crow’s feet pattern have been implemented in two phase 3 trials, suggesting it may be possible to administer 24 units in two different injection configurations into three sites per side.53,54 The first injection point is 1.5 to 2.0 cm temporal to the lateral canthus, with the second and third injection points located 1.5 to 2 cm above and below the first injection point, respectively, at an approximate 30-degree angle medially for central, upper, and full crow’s feet fan patterns. For the lower-fan crow’s feet pattern, the first injection point is the same as described above. The second and third injection points are below the first one, made in an angled superoposterior to anteroinferior line. For the lowermost injection point, a line is drawn vertically from the lateral canthus and superior to the maxillary prominence. The anteroinferior injection is made just lateral to this line. The third injection is positioned at the midpoint along a line connecting the superoposterior and anteroinferior injection points.55
Precautions, pearls, and pitfalls Beware overtreatment of lateral canthal rhytides with botulinum toxin in order to avoid creating an unusual smile with a shelf-like appearance and overprojection of the cheeks anteriorly.
Sequential treatment over 2 separate days with BTX-A first and then HA was preferred by a global consensus group. Others feel that this approach is overly cautious and prefer to treat the same day.
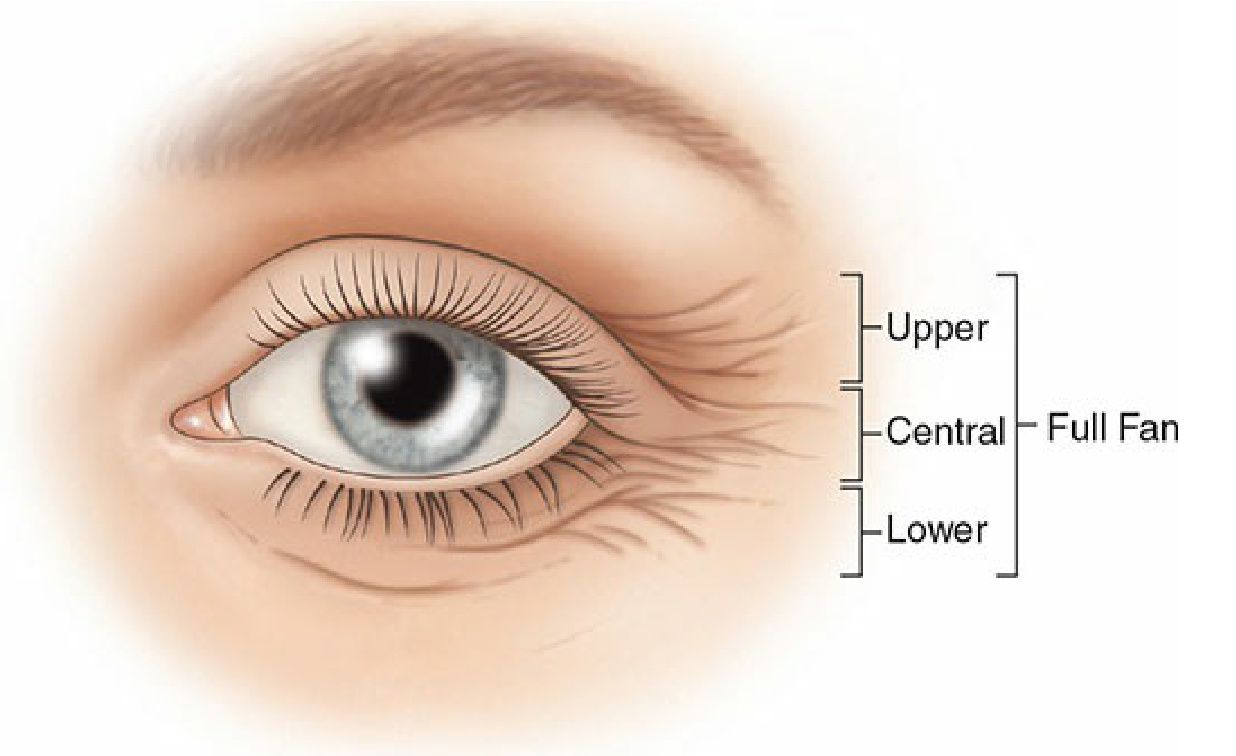
Figure 75-11. Four patterns have been described for crow’s feet; full, upper, lower, and central fan.