Fillers
Fillers
In general, HA products that integrate well into the tissue are preferable for the forehead to avoid the appearance of lumps in this area that can sometimes have thin, atrophic skin. Specific product selection will depend on patient characteristics such as the amount of subcutaneous tissue, skin thickness, and degree of lift required. A consensus group for combined HA and BTX-A treatment prefers superficial Vycross/Hylacross or dilution–reconstitution of Hylacross products for rhytides and mid-level or diluted deep volumizer Vycross for contouring.27 PLLA may also be used on the forehead, but care must be taken to use a high volume of reconstitution (14–16 mL) so as to minimize the risk of nodule formation.
It is not uncommon to see volume loss in the forehead over time. This may be manifest with mid-forehead or suprabow (especially laterally) concavity. Slight forehead convexity is aesthetically appealing and can be achieved by injecting the area of concavity to improve the appearance of forehead volume loss, giving a more convex shape and sometimes providing brow lift as a result of volume restoration.
Filler placement can also benefit lateral eye projection and attenuate contour transitions between the temple and forehead region. The goal is to achieve a gentle convex curve that is 12 to 15 degrees off the vertical as one goes from the hairline to the supraorbital prominence.12 Avoiding superficial injection of fillers that integrate poorly into tissue will minimize the risk of beading and visible overcorrection.
Forehead fillers may be injected using either a needle or cannula. When using a needle, it is placed deeply and small boluses of filler are injected in the subgaleal plane. When injecting deeply, it is important to avoid the region bounded by the midpupillary lines, the orbital rim inferiorly and a horizontal line drawn approximately 1.5 cm above the orbital rim. A cannula may also be used to inject the forehead, entering either just medial to the temporal suture line or just medial to the tail of the brow. Less experienced injectors may find this a challenging area to inject with cannulas, partially given the lack of adipose tissue and resistance to cannula movement (Figs. 75-3 and 75- 4).
Botulinum toxin The global aesthetics consensus recommends an equivalent of 8 to 25 total units of intramuscular onabotulinumtoxin A in 4 to 8 nonmicrodroplet or 8 to 20 microdroplet injection points. Injection points should be placed higher on the forehead to avoid eyebrow ptosis. Intracutaneous injections, especially near the eyebrow, can be used to achieve superficial distribution of toxin to the frontalis muscle with lower dose per unit volume of muscle to prevent eyebrow ptosis. Selection of precise BTX-A injection
points is determined by assessing frontalis muscle activity and brow movement, taking care to avoid reducing frontalis activity in areas where activity is required to keep the brows elevated and shapely. While in most cases one row of injections is adequate, more than one row may be required in individuals with tall foreheads or dynamic rhytides that extend to the frontal hairline. The lateral extent of injections is determined by the frontalis muscle width and the desire to avoid overly peaked brows (Figs. 75-5 and 75-6).
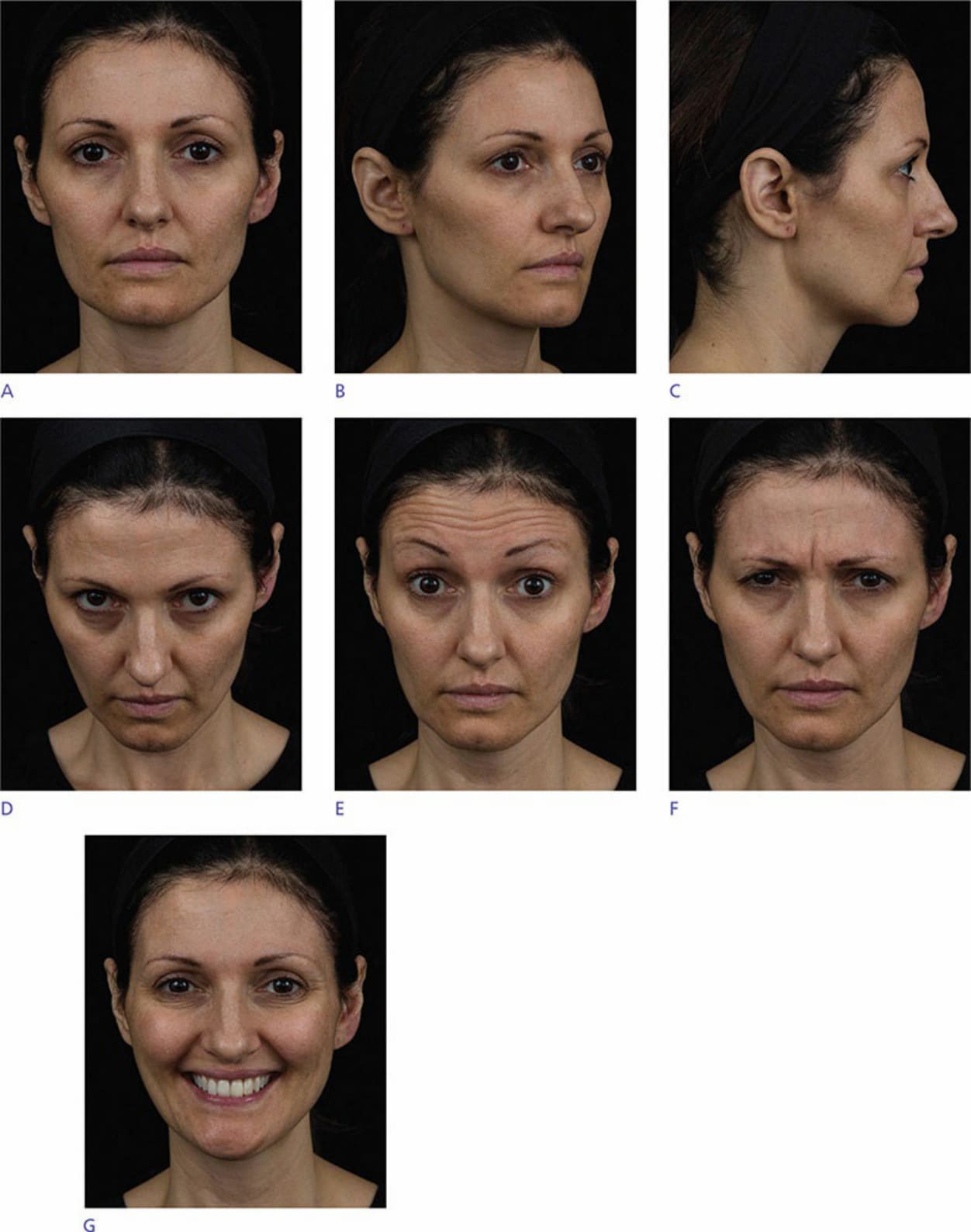
Figure 75-3. Preprocedure photographs.

Figure 75-4. After treatment with botulinum toxin in the forehead, glabella, nasalis (bunny lines), lateral canthal rhytides, and mentalis and fillers in the forehead, infrabrow hollow (A-frame deformity), cheeks (upper medial, zygomatic arch, submalar), marionette lines, lips, and angle of mandible.
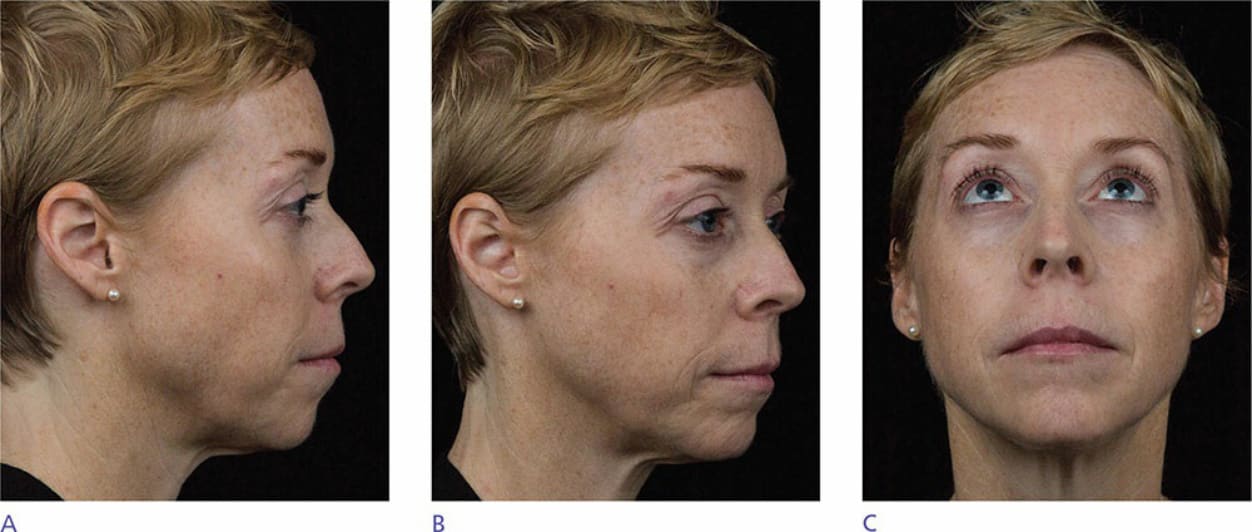
Figure 75-5. Preprocedure photographs.
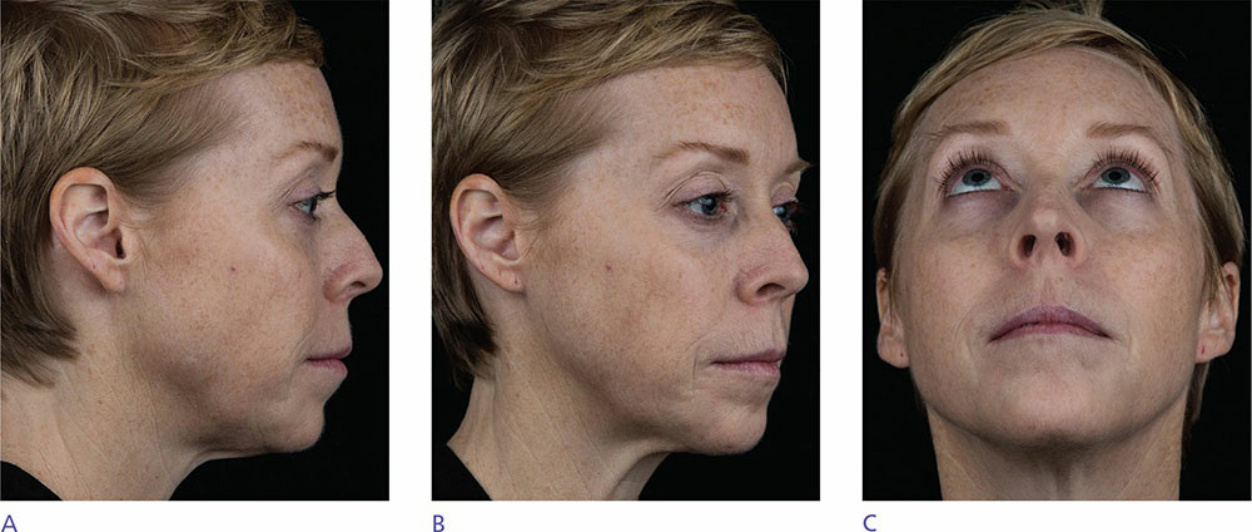
Figure 75-6. After treatment with botulinum toxin in the forehead, glabella, nasalis (bunny lines), lateral canthal rhytides, and perioral rhytides and fillers in the temples, cheeks, marionette lines, and chin.