Lower eyelid blepharoplasty
Lower eyelid blepharoplasty
The vast majority of lower lid blepharoplasty procedures are accomplished using a transconjunctival approach with canthal tightening, lower lid canthal suspension, structural fat transfer to the tear troughs, midcheek, SOOF and cheeks, and periorbital laser resurfacing. In patients with Fitzpatrick Class I-III skin, laser resurfacing is accomplished simultaneously. In patients whose skin is Class IV or above, a skin pinch excision in the presence of skin redundancy may be performed. In cases where orbicularis muscle is redundant or hypertrophic, orbicularis thermoplasty or postoperative botulinum toxin may be utilized.
Canthal tightening is performed in the majority of patients, as after laser resurfacing many patients are predisposed to developing ectropion. It is done as a preventive measure and aids in assuring good lid position in the postoperative period.
In the operating room, preoperative photographs of the patient in an upright position may be reviewed to estimate the amount of fat excess. This fat excess disappears in the supine position, particularly the temporal fat pad. It is also helpful to reference photographs of the patient at a younger age, to aid in restorative aspects of the brow, cheek, and midface.
Following intravenous sedation, the lower eyelids, lateral canthi, tear trough, and cheeks are infiltrated with a mixture of 1% Lidocaine with 100,000 epinephrine mixed with Marcaine 0.5% with 1:200,000 epinephrine (Fig. 73-33). Hyaluronidase is added, approximately 250 units per 1 cc in a 9:1 mixture.
An adequate period of time is allowed to elapse. The patient is prepped and draped in the usual sterile manner.
A corneoscleral shield is placed in the eye (Fig. 73-34). A lateral canthal incision is made 2 mm from the lateral canthus in a natural rhytid at least 5 mm from the upper eyelid incision if a concomitant upper blepharoplasty was performed. This incision measures 6 to 7 mm in length and is made through both skin and orbicularis either with a Colorado needle, a #15 blade, or a CO2 laser (Fig. 73-35). Using the pinch test (Fig. 73-36), a small amount of lower lid skin is excised (Fig. 73-37).
The assistant now grasps the tarsal edge on the conjunctival side using two Knapp rake retractors (Fig. 73-38).
An incision is made 5 mm below the inferior tarsal border as the globe is balloted forward, exposing the conjunctiva and lower eyelid retractors from approximately 2 mm medial to the caruncle to the lateral canthus (Fig. 73-39).
The lower eyelid retractors are now grasped firmly, and using a cutting cautery or a CO2 laser or gentle blunt spreading technique with an iris forcep, the orbicularis muscle is dissected from the orbital septum down to the arcus marginalis to the orbital rim. Once in the correct plane, a cotton tip applicator is used to gently dissect the orbicularis from the septum (Fig. 73-40).
A 4-0 Silk suture is placed in the lower eyelid retractor’s conjunctiva complex over the globe and a hemostat is used to clamp it to the drape (Fig. 73-41). This produces greater exposure of the inferior fat pads.
The orbital septum is opened across the entire lower eyelid, exposing the central fat pad, the nasal fat pad, and the temporal fat pad (Fig. 73-42). When necessary, the lateral retinaculum is divided, as there are two fat pads in the temporal aspect of the lower eyelid which become exposed. Using a gentle spreading technique with an iris scissor, the nasal, central, and temporal fat pads are further exposed. The fat compartments are injected with local anesthesia, clamped (Fig. 73-43), cauterized, or removed under direct visualization (Fig. 73-44). While many surgeons prefer this technique to structural fat transfer, repositioning fat below the orbital rim may result in lumps, edema and, rarely, ectropion of the eyelid. The fat is removed and partially, but not completely debulked (Fig. 73-45). The art of this technique involves what is left behind rather than what is removed.
The fat is clamped, cauterized, removed, or directly cut using a blend mixture with monopolar cautery. Hemostasis must be meticulous, and any bleeding should be controlled. The fat pads are surrounded by a capsule, which is vascular, but the fat itself
is relatively avascular, and bleeding should be minimal if the fat pads alone are resected.
A typical endpoint would involve slight visualization of the inferior orbital rim. Blotting the fat gently should allow the fat to come forward, level with the orbital rim. The temporal fat pad is slightly more aggressively debulked. The nasal fat pad is usually minimally excised.
Careful hemostasis is maintained. At this time, the 4-0 silk suture is removed. The scleral shell is removed and the eyelid is gently repositioned, verifying that there are no adhesions between the cut edges of the conjunctiva. Ectropion can occur if the eyelid is not gently repositioned in its normal anatomic position.
The analogous procedure is performed on the contralateral eye. Usually the amount of fat resected corresponds to any asymmetries—if slightly more fat is observed on one side than the other preoperatively, slightly more fat is resected.
At this time, a 4-0 Vicryl suture is used in a horizontal mattress suture to perform a lateral canthopexy (Fig. 73-46). The suture is passed from the inferior tarsal border and attached directly to the arcus marginalis. This is performed in horizontal mattress fashion. Both edges of the Vicryl suture are passed posteriorly within the orbital periosteum, aiming to reinforce the attachments of the lateral canthal tendon at Whitnall’s tubercle. The procedure is performed bilaterally and, prior to cinching the sutures, symmetry is verified.
At this time the orbicularis is closed with a single 6-0 chromic suture and the skin is
closed with multiple 6-0 fast-absorbing gut sutures.
When necessary, if chemosis supervenes from the transconjunctival approach, a 4-0 silk suture is passed as a Frost suture, which remains in place for 24 to 48 hours (Fig. 73-47).
In the course of surgery, fat transfer may be performed as well (see Chapter 61).149,150
Laser resurfacing is performed after the disposable drapes have been removed. Either fully ablative or fractional laser therapy can be used. A metal corneoscleral shield is placed in the eyes and appropriate laser precautions are taken using wet facial drapes. The lower eyelid is resurfaced using two passes. The second pass concentrates at the tear trough. If festoons are present, these are also treated aggressively with a fully ablative laser. The pretarsal lower eyelid is generally treated a single time to avoid ectropion.
The metal shields are now removed from the eyes and the areas are treated with topical Aquaphor or an occlusive dressing (Flexzan). Antibiotic ointment or antibiotic sterile ointment is instilled into the eyes.
Postoperatively, patients are treated with cool compresses.

Figure 73-33. Before beginning lower lid blepharoplasty, the lower eyelids, lateral canthi, tear trough, and cheeks are infiltrated with local anesthetic.

Figure 73-34. A corneoscleral shield is placed in the eye.

Figure 73-35. A lateral canthal incision measures 6 to 7 mm in length and is made through both skin and orbicularis either with a Colorado needle, a #15 blade, or a CO2 laser.

Figure 73-36. Using the pinch test for excision.
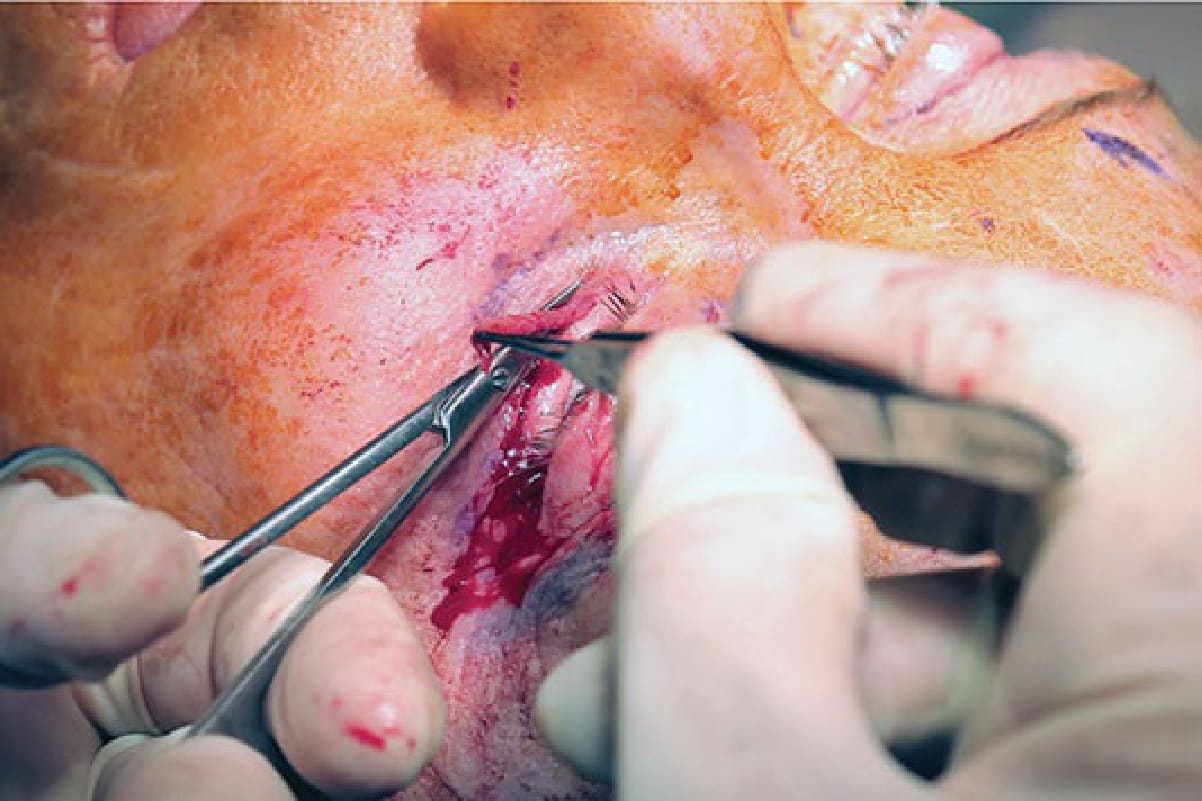
Figure 73-37. A small amount of lower lid skin is excised.
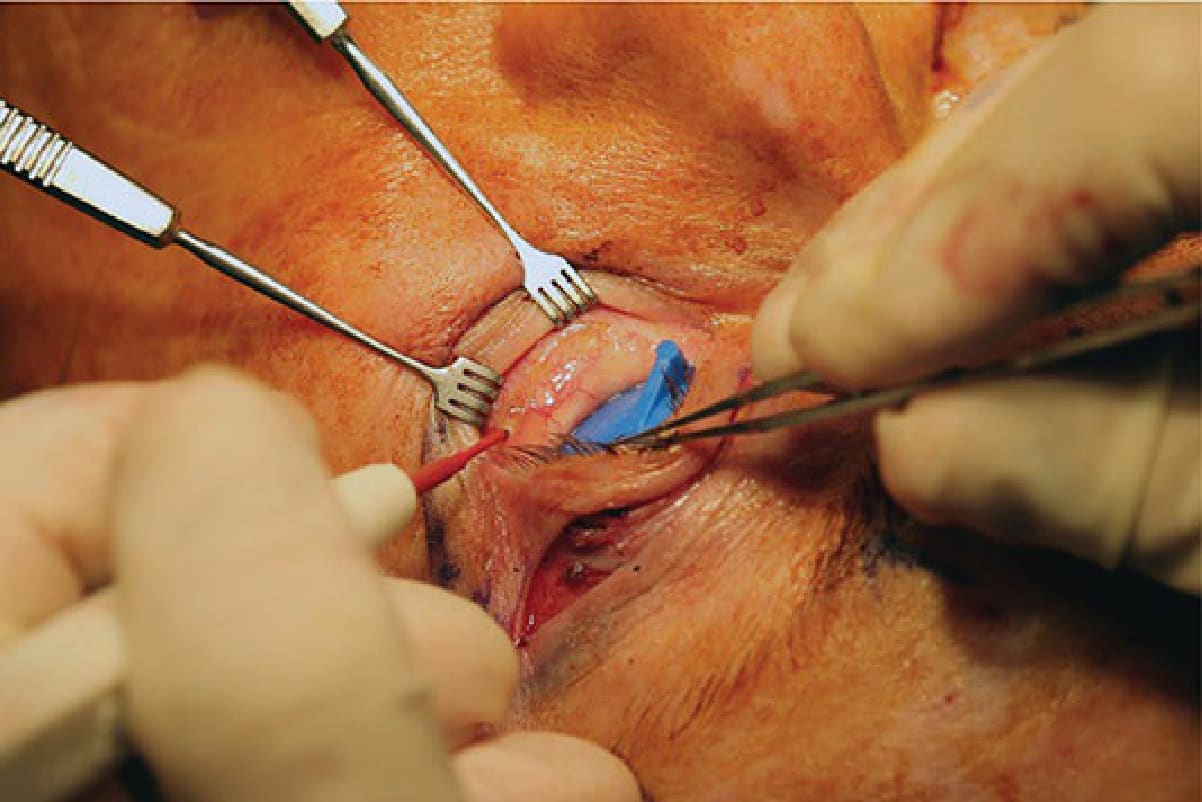
Figure 73-38. The assistant grasps the tarsal edge on the conjunctival side using two Knapp rake retractors.

Figure 73-39. An incision is made 5 mm below the inferior tarsal border as the globe is balloted forward, exposing the conjunctiva and lower eyelid retractors from approximately 2 mm medial to the caruncle to the lateral canthus.

Figure 73-40. A cotton tip applicator is used to gently dissect the orbicularis from the septum.

Figure 73-41. A 4-0 silk suture is placed in the lower eyelid retractor’s conjunctiva complex over the globe and a hemostat is used to clamp it to the drape.
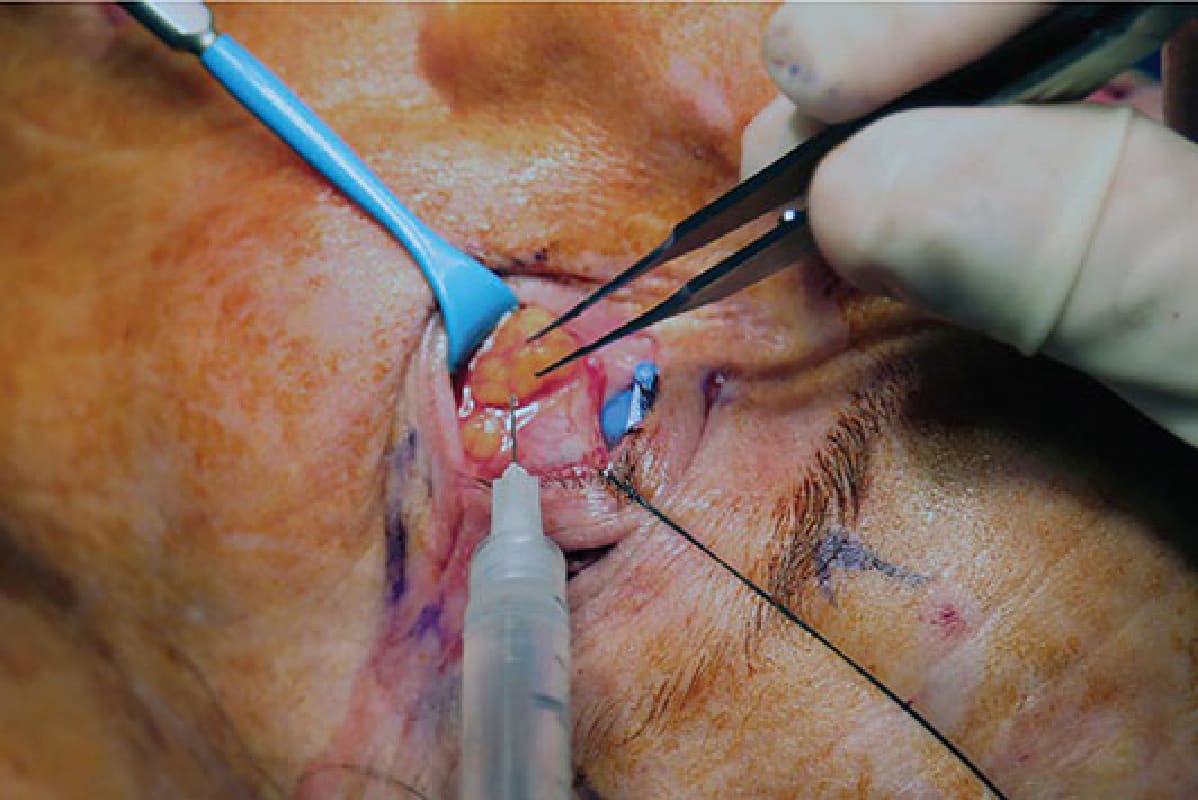
Figure 73-42. The orbital septum is opened across the entire lower eyelid, exposing the central fat pad, the nasal fat pad, and the temporal fat pad.

Figure 73-43. Using a gentle spreading technique with an iris scissor, the nasal, central, and temporal fat pads are further exposed. The fat compartments are injected with local anesthetic and clamped.

Figure 73-44. The fat compartments are injected with local anesthesia, cauterized or removed under direct visualization.

Figure 73-45. The fat is removed and partially, but not completely, debulked.
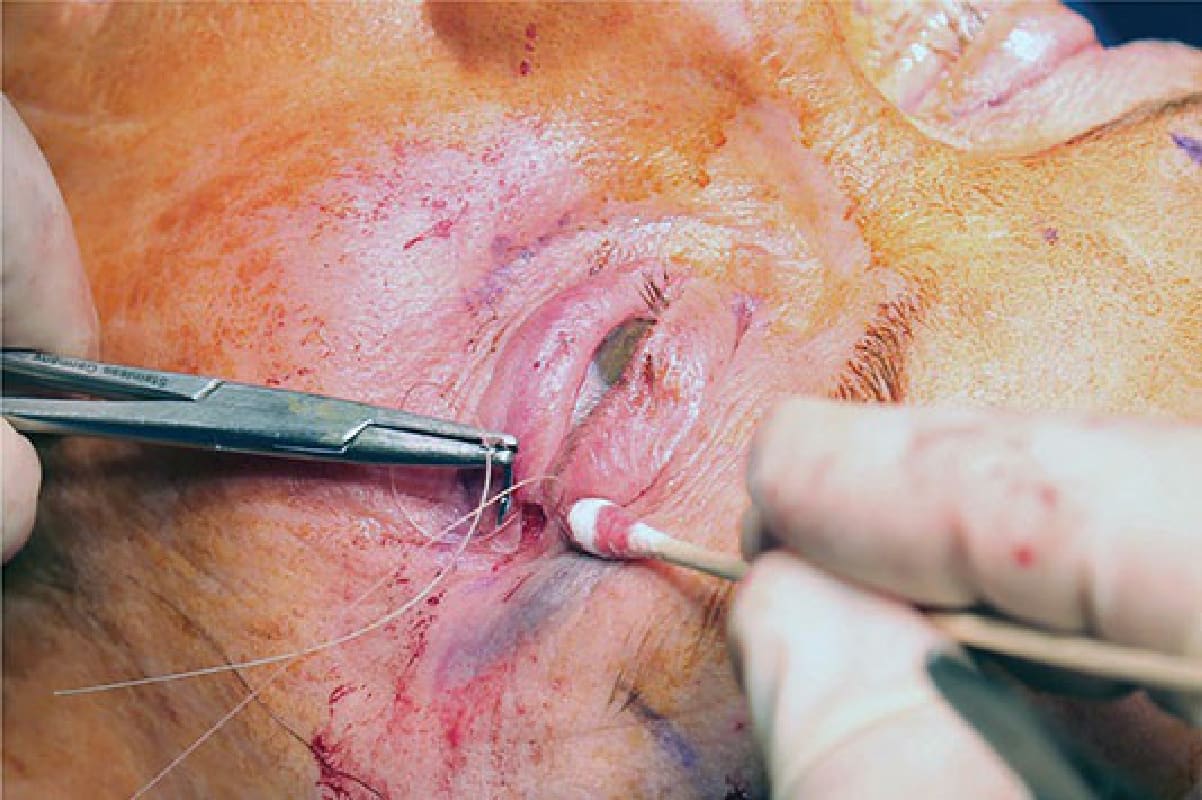
Figure 73-46. A lateral canthopexy is performed by placing a horizontal mattress suture with a 4-0 Vicryl suture.

Figure 73-47. If chemosis supervenes from the transconjunctival approach, a 4-0 silk suture is passed as a Frost suture, which remains in place for 24 to 48 hours.