Upper Eyelid Blepharoplasty
Upper Eyelid Blepharoplasty
The procedure can be tailored to the individual based on their gender and the location of their upper eyelid crease. In Asians, a discussion must occur preoperatively and special attention must be paid to the location of the crease. Most Asians will not wish to have Westernization of the eyelid crease, but may wish to have a double eyelid—a lid crease, which is placed much lower on the pretarsal eyelid.
Following intravenous sedation, Tetracaine drops (Alcon, Forth Worth, TX) are instilled into both eyes.
The eyelid crease is drawn in the operating room in the supine position with a finetipped marking pen, and symmetry is assessed using calipers (Viscot, Ultrafine, Alimed, Dedham, MA). An attempt is made to keep the eyelid crease in its original anatomic location, based on the patient’s examination and on the location of the lid crease in youth (Fig. 73-21). In the absence of a clear eyelid crease, the lid crease can be marked centrally at 10 mm in women and 8 mm in men. If skin excess is apparent, the brows are retracted upward by the surgeon or assistant to facilitate accurate lid crease marking. Medially, in the vicinity of the punctum and canalicular eyelid, the proposed incision is drawn slightly higher than the natural lid crease to prevent web formation. Laterally, the crease is extended to a line drawn that intersects the ala nasi and the lateral canthus. Beyond this, the incision is drawn in a slightly upward direction following a natural smile line no further than the lateral orbital rim.
If a brow lift is not being performed, the upper limits of skin excision are also drawn. Using a forceps and a pinch technique, skin of the upper eyelid is grasped gently and pulled upward as the proposed area of maximum skin excess is drawn in a downwards direction. Any eversion of the upper eyelid indicates that too much skin is being excised, and less skin should be placed within the confines of the markings. This procedure is performed across the entire eyelid. Slightly more aggressive excision laterally can be accomplished. Nasally, over-excision can result in abnormalities of eyelid closure and web formation.
In patients with severe dermatochalasis, and in whom the brow skin could be sewn to the lid crease because of the degree of skin excess, the surgeon should be conservative and leave at least 1 cm of infrabrow non–hair-bearing skin unresected on the upper eyelid (Fig. 73-22). Brow lift should be considered concomitantly, or the patient should be made aware that they will continue to have the appearance of skin excess due to brow ptosis.
If a brow lift is to be performed, the pinch test is omitted. Once the brow position has been set by the brow lift using a fixation technique, the amount of skin excess can be judged by gently draping the redundant skin over the eyelid crease incision with the eye closed.
Once appropriate markings have been made, the upper eyelids are infiltrated with a mixture of lidocaine 1% with 100,000 epinephrine mixed with Marcaine 0.5% with 1:200,000 epinephrine. Hyaluronidase can be added in a 9:1 mixture and aids in diffusion of the anesthetic (Fig. 73-23).
A satisfactory period of time is allowed to elapse for epinephrine effect and analgesia. The patient is then prepped and draped in the usual sterile manner.
Using a #15 blade, a CO2 laser, or a Colorado needle on pure cut mode, a lid crease incision is made (Fig. 73-24), deepened through orbicularis muscle, and the skin muscle flap is raised exposing the orbital septum (Fig. 73-25). This approach allows the surgeon to modify the amount of skin removed after fat reduction or mobilization to assure an aesthetic result.
The orbital septum is now opened centrally and across the eyelid. The central fat pad above the levator aponeurosis is immediately visualized (Fig. 73-26). The surgeon should strive to stay relatively superior so as to avoid inadvertent injury to the levator aponeurosis. The fat effectively protects the levator aponeurosis and serves as a
landmark that can prevent injury to the aponeurosis. The septum is opened after buttonholing medially and in a slightly superior direction under the orbicularis muscle.
A gentle spreading technique is employed using an iris scissors to expose the nasal fat pad (Fig. 73-27).
The nasal fat pad is injected with local anesthetic (Fig. 73-28). The fat pad can be clamped (Fig. 73-29), cauterized (Fig. 73-30) and removed, repositioned using absorbable suture, or partially debulked and sutured to any concavities that exist in the upper sulcus.
The central fat pad is minimally trimmed, if ever. This is accomplished with a scissors, and monopolar or bipolar cautery may be used to control bleeding. Lacrimal gland prolapse, if present, is treated using a 6-0 Vicryl horizontal mattress suture, securing the orbital lobe of the lacrimal gland within the lacrimal gland fossa.
The skin and/or muscle is now gently redraped over the upper eyelid. All redundant skin can be excised (Fig. 73-31). The eyelid must remain closed and the amount of skin excess can be tailored to allow for the removal of skin or skin muscle, allowing the eyelid to close completely, assuring that it will close postoperatively.
Hemostasis is verified with the monopolar cautery. The analogous procedure is performed on the contralateral side. All preoperative assymmetries are noted and fat debulking is titrated according to the preoperative evaluation as well as to what becomes apparent at the time of surgery.
The excised upper eyelid skin that is excised along with the fat may be photographed, so as to have a record of what was removed at the time of surgery. This maintains an operative record, helps the surgeon gain experience especially when viewing the postoperative result, and allows the patient to become aware of the typically minimal amount of tissue that is removed to achieve an aesthetic result.
The skin is now reapproximated, attaching the pretarsal skin edge directly to the levator aponeurosis in three locations using a 6-0 absorbable Vicryl suture (Fig. 73-32). The remaining skin is closed with a 6-0 Prolene suture either in running fashion or in subcuticular fashion.
Ointment is placed in the eyes and on the incisions. The drapes are removed. If planned, lower eyelid surgery can now be accomplished.

Figure 73-21. The eyelid crease.

Figure 73-22. In patients with severe dermatochalasis, and in whom the brow skin could be sewn to the lid crease because of the degree of skin excess, the surgeon should be conservative and leave at least 1 cm of infrabrow non– hair-bearing skin unresected on the upper eyelid.

Figure 73-23. The upper eyelids are infiltrated.

Figure 73-24. A lid crease incision is made.

Figure 73-25. The skin muscle flap is raised, exposing the orbital septum.
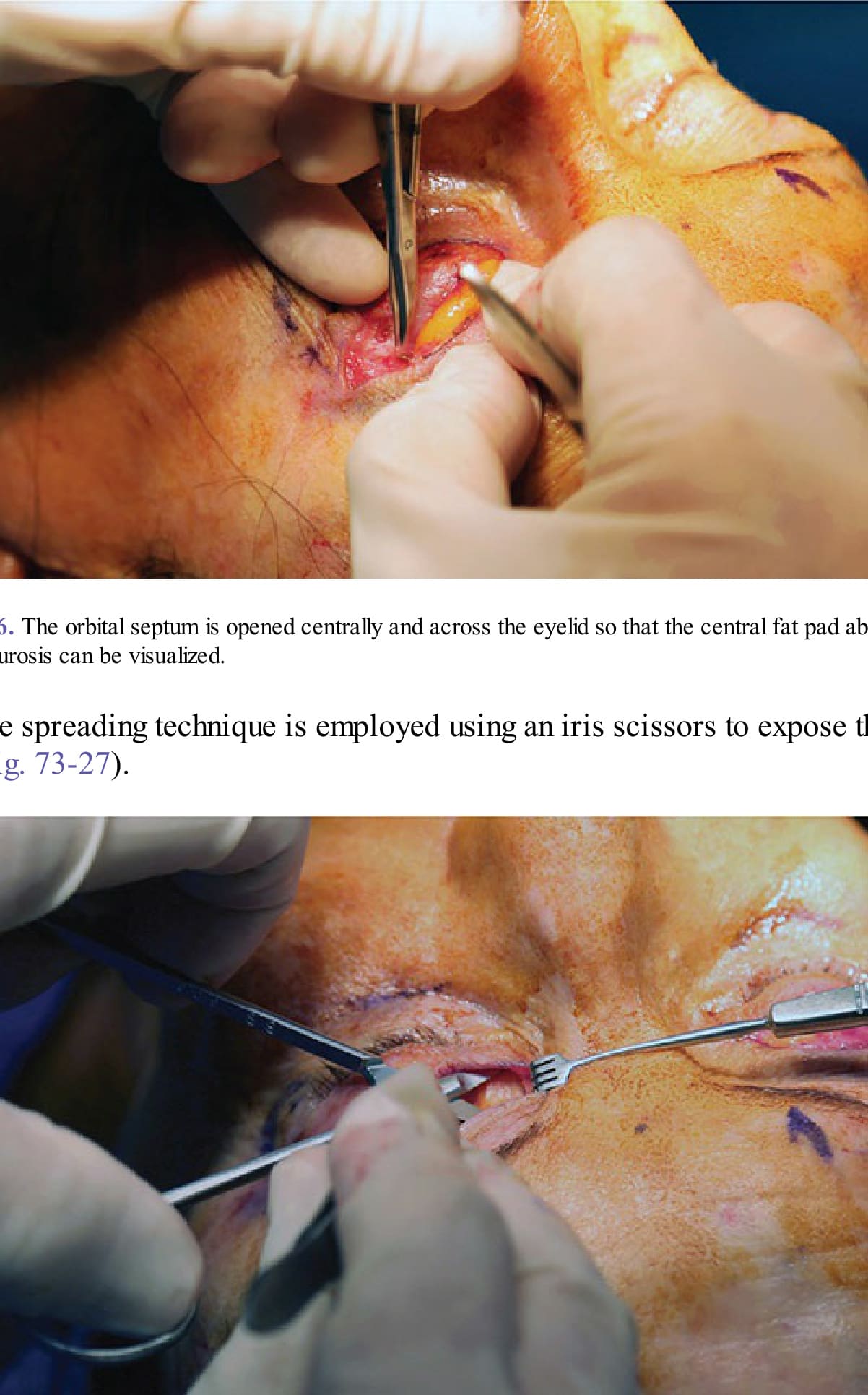
Figure 73-26. The orbital septum is opened centrally and across the eyelid so that the central fat pad above the levator aponeurosis can be visualized.

Figure 73-27. A gentle spreading technique is employed using an iris scissors to expose the nasal fat pad.
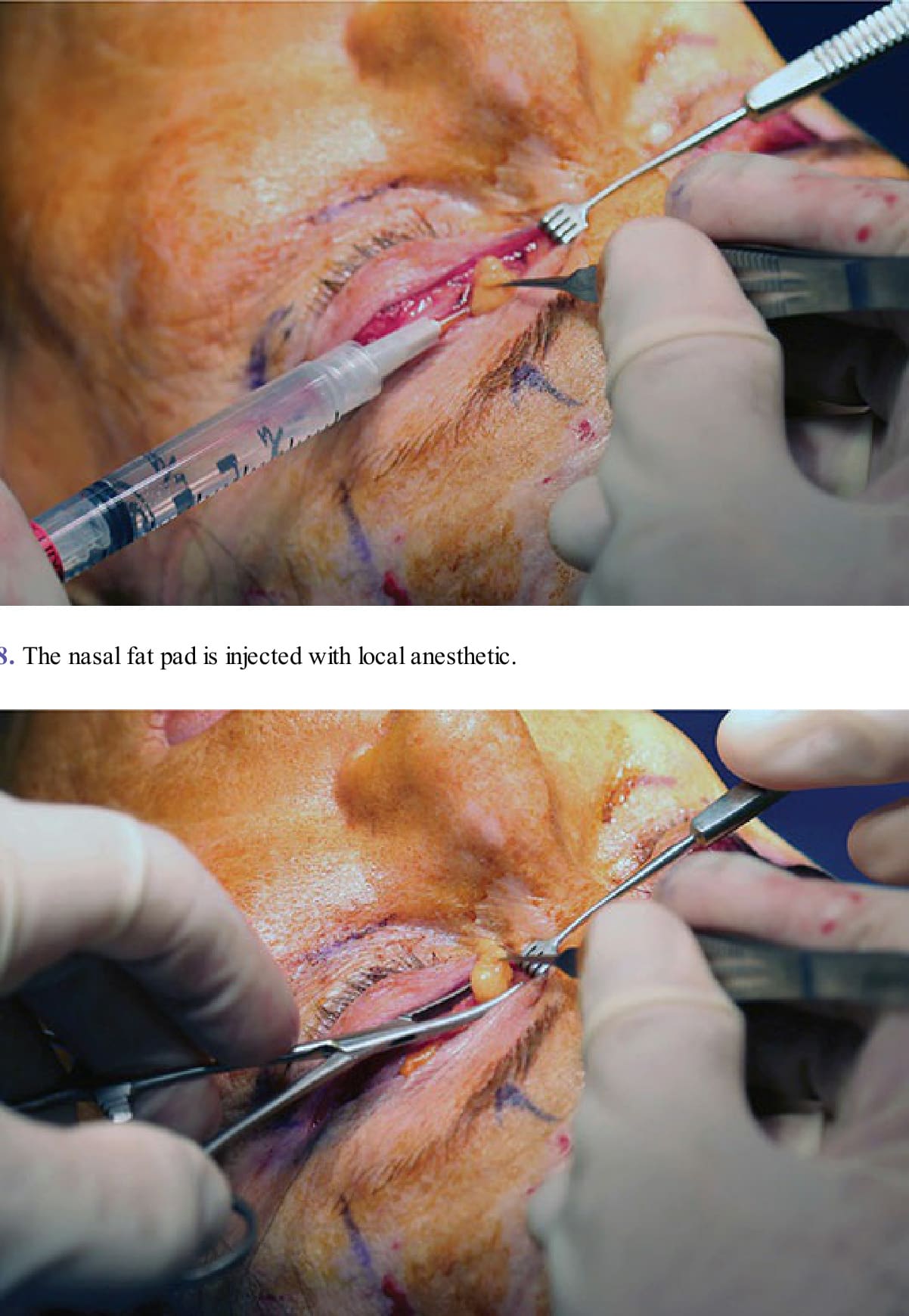
Figure 73-28. The nasal fat pad is injected with local anesthetic.
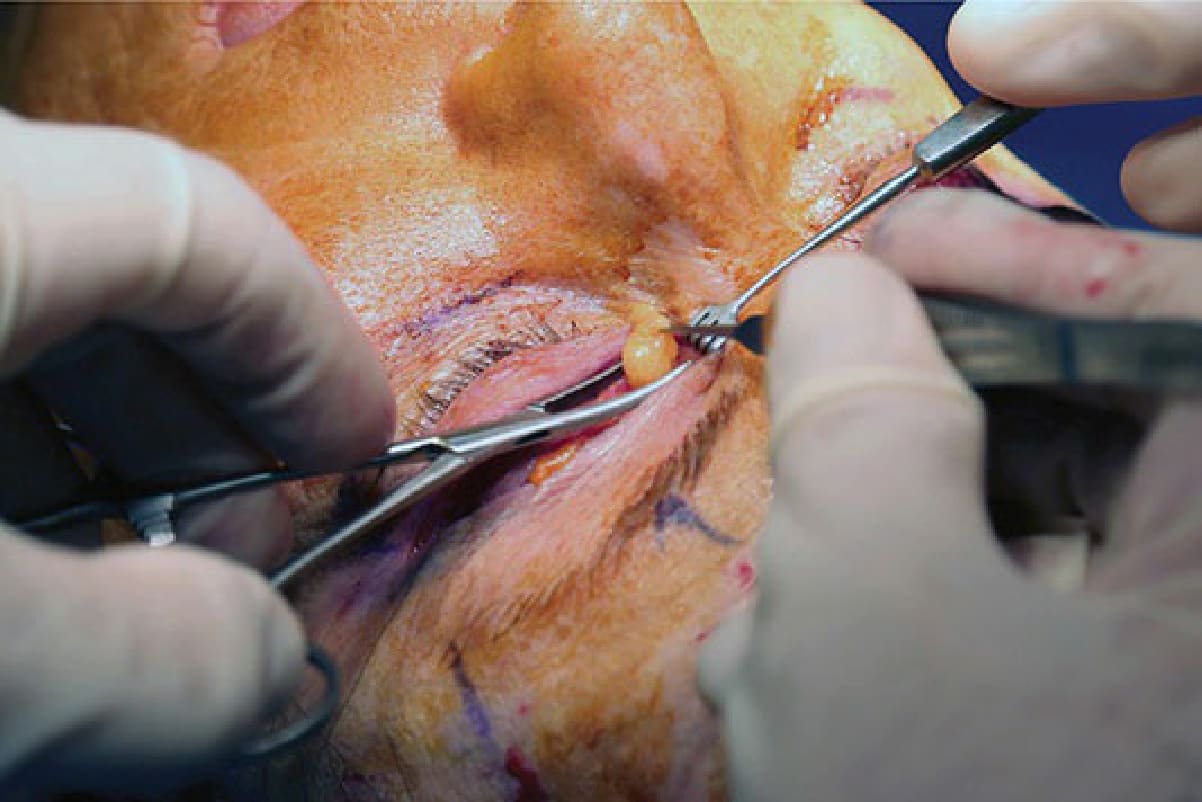
Figure 73-29. The nasal fat pad can be clamped.
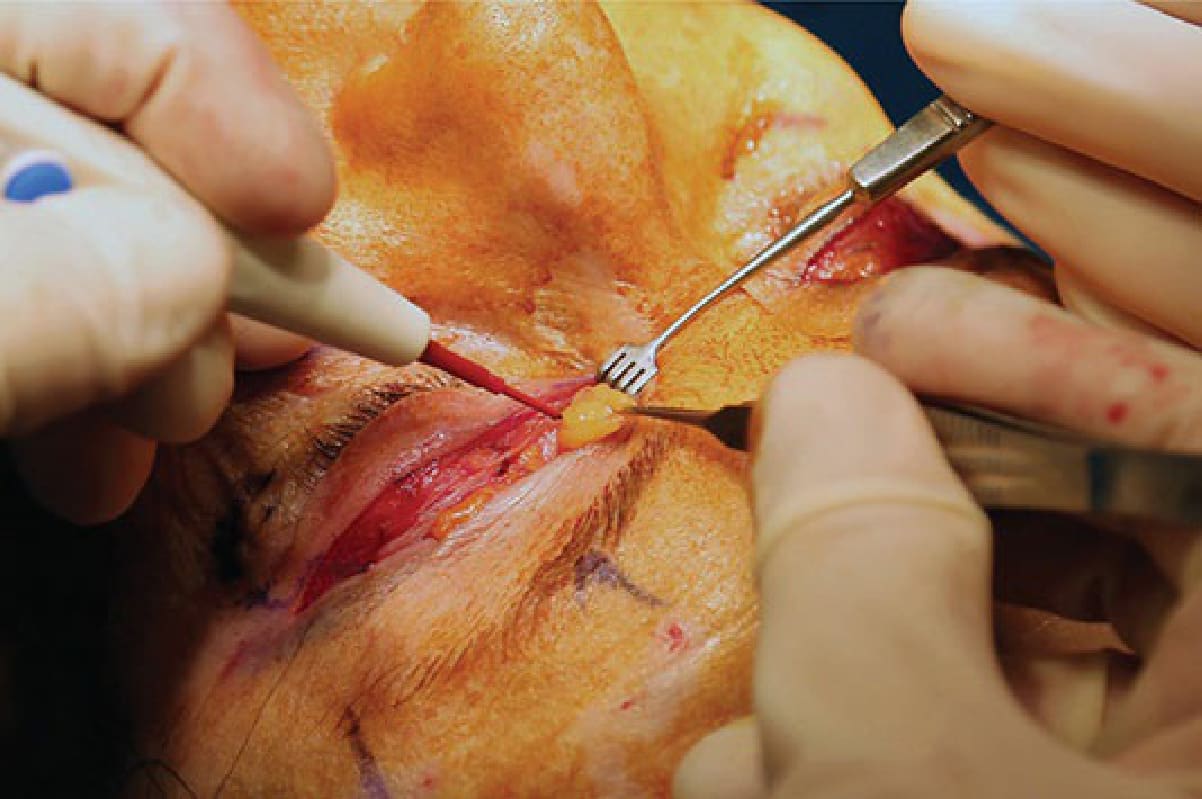
Figure 73-30. The nasal fat pad can be cauterized.

Figure 73-31. The skin and/or muscle is gently redraped over the upper eyelid and all redundant skin can be excised.

Figure 73-32. The skin is reapproximated, attaching the pretarsal skin edge directly to the levator aponeurosis in three locations using a 6-0 absorbable Vicryl suture.