POSTOPERATIVE CARE
POSTOPERATIVE CARE
There are a range of postoperative regimens for upper and lower lid blepharoplasty, but very few evidence-based guidelines for postsurgical management. Cooling with ice packs is often advocated, though there is no clear evidence that cooling is helpful. Pool et al. performed a randomized study of 38 upper lid blepharoplasty patients for whom one eyelid was cooled postoperatively with ice packs and their other eyelid was untreated.122 They found significantly lower pain scores on day 1 in the cooled eyelid, but no differences between groups in terms of lid edema, erythema, or hematoma formation. While there was a difference in pain, overall pain scores were low, leading them to conclude that the recommendation of a postoperative cooling regimen could be abandoned. There is also evidence that inappropriate use of ice packs can lead to unintentional damage of delicate eyelid skin.123
Other technologies have been explored to decrease postoperative pain, edema, and erythema. Pulsed electromagnetic energy has been studied in the context of wound healing, and may be beneficial for postoperative symptoms. Czyz et al. used ActiPatch, a device that emits low-level pulsed electromagnetic energy, on upper lid blepharoplasty patients.124 While there were no objective differences in postoperative symptom grades, patients subjectively felt that the appearance of edema and ecchymoses was initially better on the ActiPatch side. However, the patch was not user friendly, difficult to apply, and resulted in a small skin burn in two patients at the adhesion site because of improper application.
Intensed pulse light (IPL) systems use flash lamps and computer controlled capacity banks to generate pulsed polychromatic high-intensity light across a range of different wavelengths. IPL has been used to treat facial hair, vascular lesions, pigmented lesions, acne, redness, and photoaging. In a recent prospective, randomized, double-blinded, controlled trial the effect of IPL on postoperative ecchymoses was examined.125 Twenty eight patients were enrolled who had a variety of oculofacial procedures in which one side of their face was treated with IPL therapy postoperatively and the other side was
treated with the normal postoperative regimen. In the early postoperative period, there was a significant reduction in the severity and color of ecchymoses on the IPL treated side, but the difference equalized after about 12 days postoperatively.
Hemostasis is a crucial part of eyelid surgery and postoperative wound healing. Apart from standard intraoperative use of cautery, which can be associated with tissue damage, there are few modalities available to alter the appearance of ecchymoses in the postoperative wound healing period. Kaolin is a mineral that has been effective in other areas of medicine at controlling hemorrhage when combined with gauze and applied to a surgical wound. Kondapalli et al. looked at kaolin embedded intraoperative gauze application to upper eyelid blepharoplasty wound beds and assessed the degree of postoperative inflammation and ecchymosis.126 While there were no significant differences in intraoperative bleeding or postoperative edema, Kaolin application did result in a significant reduction in ecchymosis at postoperative days 4 and 7.
Arnica is a flowering herb that has been shown to reduce postsurgical edema and ecchymosis. While Seeley et al. found it to reduce the incidence of ecchymosis in facelift surgery,127 its use in periorbital surgery has recently been explored with two well-designed, prospective, randomized, double-blinded studies.128,129 Both independent research teams found that there was no significant difference in postoperative pain, edema, or ecchymosis between arnica and nonarnica treated eyelids after upper lid blepharoplasty. A systematic review of the literature on the effectiveness of arnica in wound healing found similarly disappointing results with its use in other parts of the body.130
COMPLICATIONS
Blepharoplasty, when performed correctly, is very safe and produces rewarding results. However, it can have devastating complications related to both vision loss and cosmetic deformity. Complications can be divided into two groups: (1) errors in preoperative measurements and (2) surgical errors.
When deciding how much skin to remove in upper lid blepharoplasty, a conservative approach is essential. The consequences of aggressive skin removal are more difficult to correct than the consequences of managing residual skin excess. Up to 5% to 10% of patients may need additional skin removal after blepharoplasty surgery.15 It is important to counsel patients that the need for additional skin removal should not adversely influence an overall successful cosmetic outcome. Residual skin excess usually results from underestimation of how much skin is present, and usually manifests with persistent temporal hooding. If there is residual dermatochalasis after blepharoplasty, the surgeon should always check the eyebrow position to ensure that there is not concomitant brow
ptosis before consideration of further skin removal. If the surgeon does not agree with further skin removal despite a patient’s wish for additional surgery, efforts should be made to explain proper lid function and the need for at least 20 mm of anterior lamella. Ultimately, one should wait at least 3 to 6 months before considering additional surgery.
Eyelid ptosis can occur after blepharoplasty as a result of unrecognized preoperative ptosis or due to inadvertent injury to the levator muscle during surgery. The upper eyelid height should always be checked preoperatively, and a preoperative discussion about expectations is essential to avoid postoperative disappointment. Early postoperative mechanical ptosis from surgical edema is not uncommon. However, if ptosis persists beyond the normal healing time, the levator muscle may have been traumatized during blepharoplasty surgery. For this reason, a strong knowledge of anatomy is necessary in blepharoplasty surgery to avoid injury to delicate eyelid structures.
As with all cosmetic procedures, patients expect postoperative symmetry. However, some patients will notice asymmetry postoperatively that was present preoperatively, which is why high-quality preoperative photos are essential. An asymmetric upper lid crease is an unfortunate complication that can be avoided with good preoperative measurements. The skin markings are perhaps the most important step in achieving postoperative symmetry. Calipers should be used to obtain precise measurements. The natural lid crease should be used as the inferior border of the incision. If the lid crease is poorly defined or absent, standard guidelines for the Caucasian (7–8 mm for a man; 8–10 mm for a woman) and Asian eyelids (5–6 mm for a man; 6–7 mm for a woman) should be used.131 Slight early postoperative asymmetry may occur, but if this is persistent, surgical revision may be necessary. Overall, it is easier to raise a crease rather than to lower it.132 If a higher crease needs to be created, a new incision should be made at a higher location with crease reforming sutures to fixate underlying orbicularis to levator muscle. If a lower crease needs to be created, an incision should be made at the lower level with advancement of preaponeurotic fat or through the use of free fat pearls to prevent adhesion at the higher level.
One of the most common complications of lower lid blepharoplasty is retraction, causing frank ectropion or a rounded lateral canthal appearance (Fig. 73-20). This can be cosmetically disturbing and highly symptomatic from dry eye–related irritation. This kind of eyelid malposition often results from scarring of the middle lamella and/or aggressive skin removal, typically in the setting of unrecognized lower lid laxity. It is paramount to avoid excessive skin removal; usually only 2 mm of skin excision is required at the most.15 It is also important to explain to patients preoperatively that the goal of lower lid blepharoplasty is to improve lid contour, not to remove skin. Skin peeling or laser resurfacing should be used to address excessive lower lid skin, rather than direct skin excision. The treatment of lower lid retraction can be difficult, usually requiring surgical release of middle lamellar scarring and grafting with hard palate, fat,
or acellular dermis.18,131–133 Skin grafting to the anterior lamella should be used as a last resort. Often, the final outcome of lower lid retraction repair is suboptimal.
Lagophthalmos, or inability to close the eyelids, can be a highly problematic complication after blepharoplasty (Fig. 73-13). Not only is it uncomfortable, but it can place the health of the cornea in jeopardy. Lagophathalmos can occur as a result of various causes, including excessive skin excision, excessive orbicularis oculi resection, postoperative orbicularis weakness, or lid retraction. Prior LASIK surgery, in particular, may place the cornea at risk even with very minimal lagophthalmos.134 Early lagophthalmos from edema, decreased effort secondary to pain, or orbicularis oculi dysfunction is common and usually resolves with time. Artificial tears and ointments can be used to protect the ocular surface in the short-term. Usually 2 mm or more of lagophthalmos is symptomatic and, if persistent, may require surgical correction.
Inadvertent globe penetration during local anesthetic infiltration of the eyelid is a rare occurrence, but has been reported in the literature.135,136 This complication can be avoided using several techniques. While awake patients do not tolerate scleral shells well, a shell can be used in a patient having blepharoplasty surgery under general anesthesia to cover and protect the globe. Additionally, several modifications to injection technique can reduce the risk of this occurring. The injection needle tip should
always be directed away from the globe. Once the needle is engaged in the subcutaneous space, the lid should be lifted up off the globe for the duration of the injection. A small amount of anesthetic volume should be injected to create a fluid wave which will separate the subcutaneous tissues and create a pocket through which to continue advancing the injection needle.
Small amounts of hemorrhage are to be expected with any surgery, and often lead to postoperative bleeding. During the injection of local anesthetic, efforts should be made to avoid visible vessels. If a small hematoma begins to develop, pressure can be applied to the area intraoperatively to minimize postoperative ecchymoses. Patients should be counseled preoperatively regarding the risk of bruising so as to minimize postoperative concerns. If hemorrhage is diffuse, a preseptal hematoma can occur. This is usually associated with a tense, swollen, and ecchymotic lid. It is essential to check for retrobulbar hemorrhage in these situations. In contrast to a retrobulbar process, if the hemorrhage is isolated to the preseptal space, there is usually minimal or absent associated pain. Anterior hematomas are best managed conservatively with elevation of the head of the bed, ice, direct pressure compresses, rest, and close observation. Since evacuation of a preseptal hematoma can lead to recurrent bleeding, drainage is usually not necessary. This complication is very concerning to patients because it delays healing and is unsightly. However, it is important to reassure an affected patient that it rarely causes loss of vision and does not affect the final aesthetic outcome.
Retrobulbar, or postseptal, hemorrhage is one of the most feared complications of blepharoplasty surgery. Although it is rare, occurring at an incidence of 0.055%,15 it can lead to permanent vision loss. Retrobulbar hemorrhage usually occurs in the early postoperative period (within 24 hours of surgery), but vision loss from hemorrhage has been reported up to 9 days after surgery.137 Minimizing strenuous postoperative activity for at least 10 days after surgery is recommended. Bleeding usually comes from an arterial source and can occur anteriorly with posterior extension through a septal opening or can start as a primary posterior process. The orbital cavity measures about 30 mL, and there is little room for expansion within this bony space. Blood collection within the orbit can cause compartment syndrome with symptoms of pain, proptosis, limitation of extraocular muscles, elevated intraocular pressure, an afferent pupillary defect from optic nerve compromise, and ultimate vision loss from retinal ischemia. While permanent vision loss occurs only 0.045% of the time,138 retrobulbar hemorrhage is an ophthalmic emergency. Diagnosis of a hemorrhage should be made on a clinical basis and time should not be wasted obtaining an imaging scan. The surgical wound should be explored and the culprit vessel cauterized. Immediate lateral canthotomy and inferior cantholysis of the lateral canthal tendon should be performed if an obvious bleeding source is not visualized or if a delay will not allow a return to the operative setting. Successful release of the lower lid is evidenced when the lateral lid can be
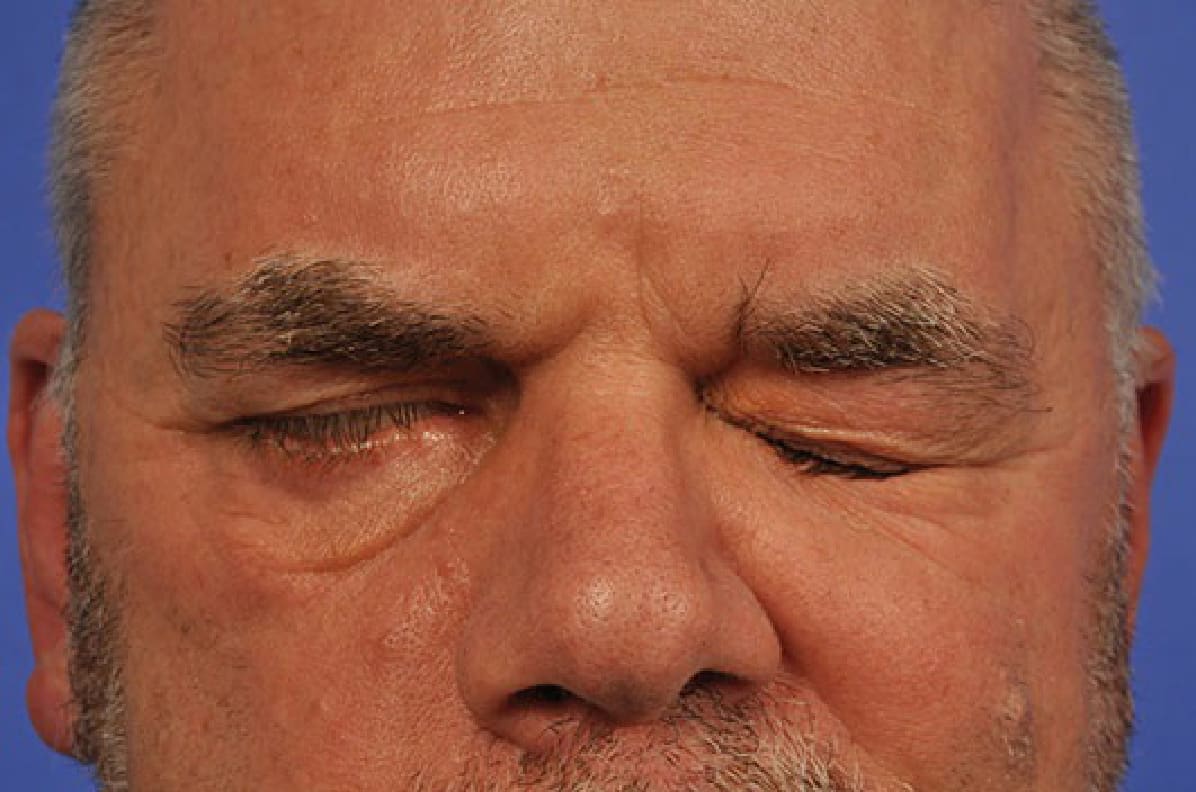
Figure 73-13. Unilateral lagophthalmos.

Figure 73-20. Postblepharoplasty lower lid retraction.