EVALUATION
EVALUATION
Blepharoplasty is a procedure of nuance, and preoperative evaluation sets the groundwork for effective surgical intervention. An understanding of the typical changes seen in the aging face is important (Fig. 73-10).
The first step in the evaluation is the history. The surgeon should gain an understanding of what is most bothersome to the patient about their eyelid and facial appearance. For example, the surgeon must understand if their patient’s dissatisfaction lies in excess skin (“bags”), hyperpigmentation (“circles”), fat prolapse (“puffiness”), rhytides, and/or ptosis in order to generate a plan that will ultimately lead to patient satisfaction. A combination of these issues brings the patient to seek surgical intervention. Motivation for surgery should be discussed. Often a major event, such as the wedding, will affect the timing of surgery.
A complete past medical history should be obtained including any chronic illnesses such as hypertension, heart disease, diabetes, obesity, blood dyscrasias, thyroid disorders, and autoimmune conditions (especially those requiring immunosuppressive medications), all of which might increase anesthesia risk, bleeding risk, and postoperative wound healing time. Active medications should be recorded with
particular attention to those that may affect clotting, such as dietary supplements (i.e., fish oil, garlic, ginko, ginger, ginseng, glucosamine), over-the-counter pain medications (i.e., Advil, Aleve, Aspirin), and anticoagulants. These should all be stopped at least 2 weeks preoperatively.26 Medication allergies should also be documented. A complete social history should be obtained, including smoking, alcohol intake, and illicit drug use, all of which may lead to poor wound healing or poor perioperative compliance. Other important aspects of the social history include patient occupation and job requirements, since time off from work will be necessary.
A detailed ocular and periorbital history is necessary for appropriate surgical counseling, including prior oculofacial, refractive, or orbital surgery, trauma, glaucoma, epiphora, contact lens use, and dry eye syndrome. LASIK (laser assisted in situ keratomileusis), a refractive procedure performed for the correction of myopia or hyperopia, is a specific consideration. Patients who have had LASIK surgery often have dry eye and diminished corneal sensation. LASIK surgery performed soon after blepharoplasty and blepharoplasty performed soon after LASIK surgery have resulted in corneal complications.27 As a result, waiting a period of at least 1 year between these surgeries may be wise. Dry eye is common in the general population, occurring in up to 5% to 15% of people.28 Symptoms include foreign-body sensation, blurred vision, photophobia, headache, itching, tearing, discharge, and eye redness.29 Schirmer’s strip testing is used to quantify tear production (Fig. 73-11). Fluorescein and lissamine green dye staining are used to highlight areas of corneal or conjunctival de-epithelialization from dry eye syndrome (Fig. 73-12). A high incidence of postoperative dry eye symptoms occur after blepharoplasty, and patients should be made aware of this risk as part of the preoperative discussion. However, if symptoms of dry eye are present, one may consider referral to an ophthalmologist for further evaluation before proceeding with blepharoplasty, and full informed consent with the patient regarding the risks of exacerbating dry eye and conservative surgery (or no surgery) is recommended in this subgroup.
A general physical examination should be performed. Facial examination should include an overall assessment of skin, muscle, fat, middle lamella, and bone structure. It is important to distinguish between ptosis (drooping upper eyelid) and dermatochalasis (excess upper eyelid skin). An assessment of ptosis should take into account variations in eyelid height, such as level of alertness, pharmacologic agents, direction of gaze, size
of globe, orbital volume, visual acuity, and extraocular muscle balance (position of the eye). If true ptosis is found to be present during the preoperative evaluation, consider referral to an ophthalmologist.
Brow ptosis should be distinguished from dermatochalasis. If both problems are present and blepharoplasty alone is performed, the degree of brow ptosis may be worsened. In such patients, a combined brow lift and blepharoplasty may be optimal. Additionally, the degree of eyebrow compensatory frontalis overaction should be noted. All patients have some degree of resting frontalis tone, and blepharoplasty may decrease frontalis muscle tone, resulting in brow descent and a postoperative surprise in lowered brow position.30
In the general examination, the surgeon proceeds from external (skin) to internal (bone). The surgeon must carefully document the location of skin excess. The degree of skin laxity should be noted, along with the amount of sun damage. A close evaluation of the skin should be performed, documenting the amount of sun damage and actinic changes, texture, and laxity. Skin texture should be optimized before blepharoplasty with an ideal skin care regimen. Similarly, eczema and rosacea should be treated beforehand to optimize surgical outcomes. When skin resurfacing is considered, skin type may be noted.31
Muscle tone should be evaluated, assessing the strength of lid closure and looking for the presence of festoons of the orbicularis. If there is any eyelid weakness or lagophthalmos (Fig. 73-13), a Bell’s phenomenon should be recorded, as well as evidence of cranial nerve VII palsy or aberrant regeneration.
Volume excess in the upper and lower eyelids should be documented, with details about the relative location and amount, as well as volume deflation in the facial fat compartments. Ptosis of the lacrimal gland should be noted in the temporal upper eyelid, and must not be mistaken for fat excess (Fig. 73-9). In any patient with a prominent lacrimal gland, careful inspection of the area should be performed to make sure that there is not lacrimal gland enlargement from an underlying neoplastic, inflammatory, or infectious process.
Atrophy and ptosis of the malar fat pad as well as submalar hollowing should also be noted. Asymmetry is the rule in most patients, and it is helpful during the preoperative evaluation to point this out so that the patient understands that these asymmetries will likely persist postoperatively.
When there is fat prolapse, the specific compartments that are prominent should be quantified from 1 to 3+, with the size of the small fingernail equaling one unit (Figs. 73- 14 and 73-15).32 Areas of fat atrophy and hollowing may be noted in the tear trough region, cheek-malar groove, lateral brow, and temple area.
Lower lid festoons, or malar mounds, are redundant folds of loose skin, muscle, fat and edema that extend beyond the lateral cheek. The skin is occasionally pigmented in chronic cases. Their etiology is not entirely understood. Festoons may be caused by orbicularis muscle or orbitomalar ligament weakness, allowing skin, fat, and muscle to descend below the level of the orbital rim.33 They may be more common in patients with thyroid eye disease, kidney disease, or lymphatic obstruction, and can be seen after eyelid or midface surgery.33
Finally, the configuration of the eye within the bony orbit and its relationship to the inferior orbital rim can predictably determine whether a patient may be at high risk for ectropion and dry eye symptoms after surgery. Patients with prominent eyes without adequate bony support, so-called negative vector patients, are at risk to have these issues (Fig. 73-16). While this can be roughly predicted from a general examination, a Hertel exophthalmometer can be used to make a more objective determination (Fig. 73- 17).34
The ophthalmic examination should always include a visual acuity measurement with the Snellen eye chart. Formal visual field testing may be necessary for insurance purposes. Evaluation of extraocular motility, including strabismus and pupillary light response should be performed. Marginal reflex distances (distance from central pupillary light reflex to upper and lower lid margins) (Fig. 73-18), interpalpebral fissure height, levator function, and upper eyelid crease height should also be recorded. The strength of the orbicularis muscle and lower lid retractors should be assessed with
the lower lid snap back test (normal is <1 second) (Fig. 73-19) and the eyelid distraction test (normal is when the lid does not distract more than 6 mm from the globe). The lateral canthal tendon is usually 2 mm higher than the medial canthal tendon (positive canthal tilt). A negative canthal tilt may be another sign of increased lid laxity.34 In these cases, blepharoplasty should be performed with lateral canthopexy to prevent lid malposition postoperatively (i.e., ectropion).35 Again, dry eye findings can be assessed by measuring tear secretion with Shirmer’s testing and with ocular surface staining (lissamine green and fluorescein dye) of areas of de-epithelialization as viewed under the slit lamp.
Reviewing old photographs from the distant and more recent past is helpful to accurately tailor each surgery to a patient’s individualized youthful facial features and bone structure. For example, if a patient had limited pretarsal show with low-set eyelid folds when they were younger, the surgical plan should still respect the patient’s unique premorbid appearance.16 Prior to surgery, photographs without make-up and with hair pulled back are a prerequisite, and are also helpful in discussing preoperative planning with the patient.
Most insurance companies require clinical photographs and visual field images for preapproval purposes. The methods of obtaining precertification for insurance purposes continue to evolve as the world of health care changes.
An appropriate evaluation of the eyelids and face allows the surgeon to make many decisions regarding the surgical technique that might produce the best aesthetic outcome.

Figure 73-9. Unilateral lacrimal gland prolapse.

Figure 73-10. Changes of the aging face.

Figure 73-11. Shirmer’s strip testing for dry eye evaluation.
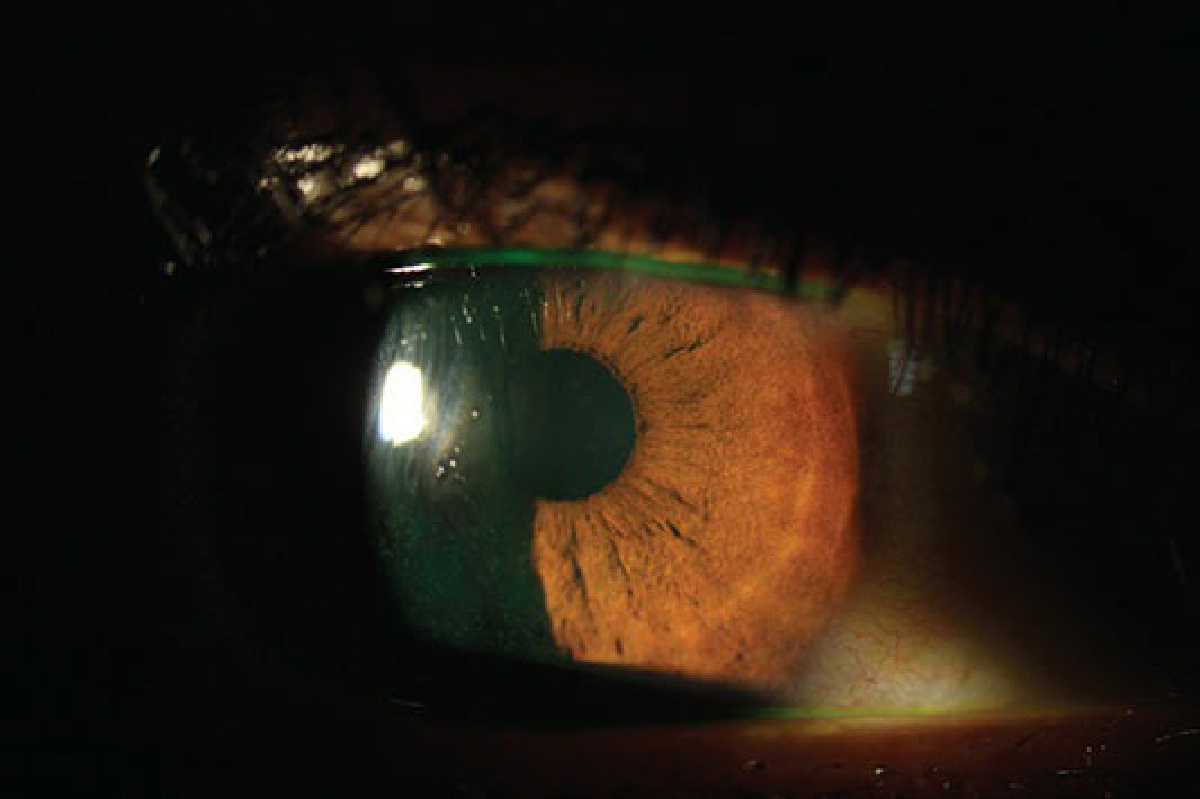
Figure 73-12. Punctate epithelial fluorescein staining (green dots) on corneal surface in dry eye syndrome.
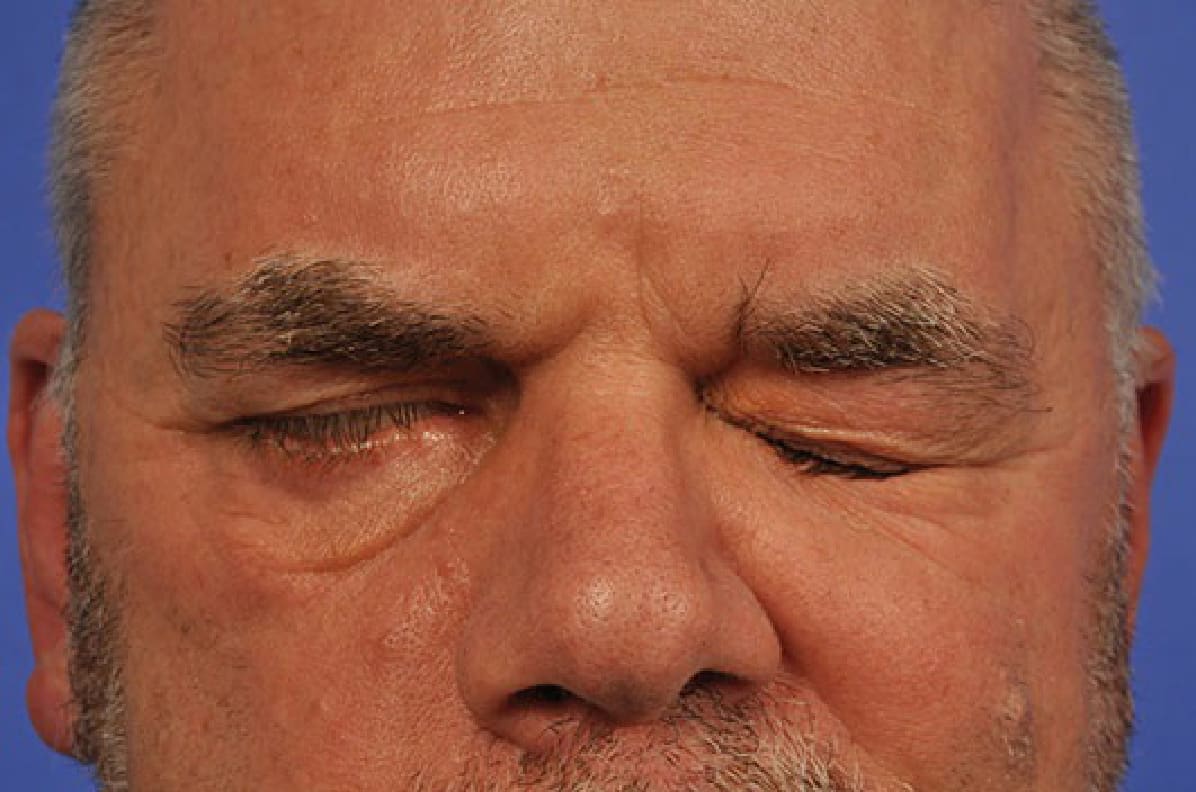
Figure 73-13. Unilateral lagophthalmos.
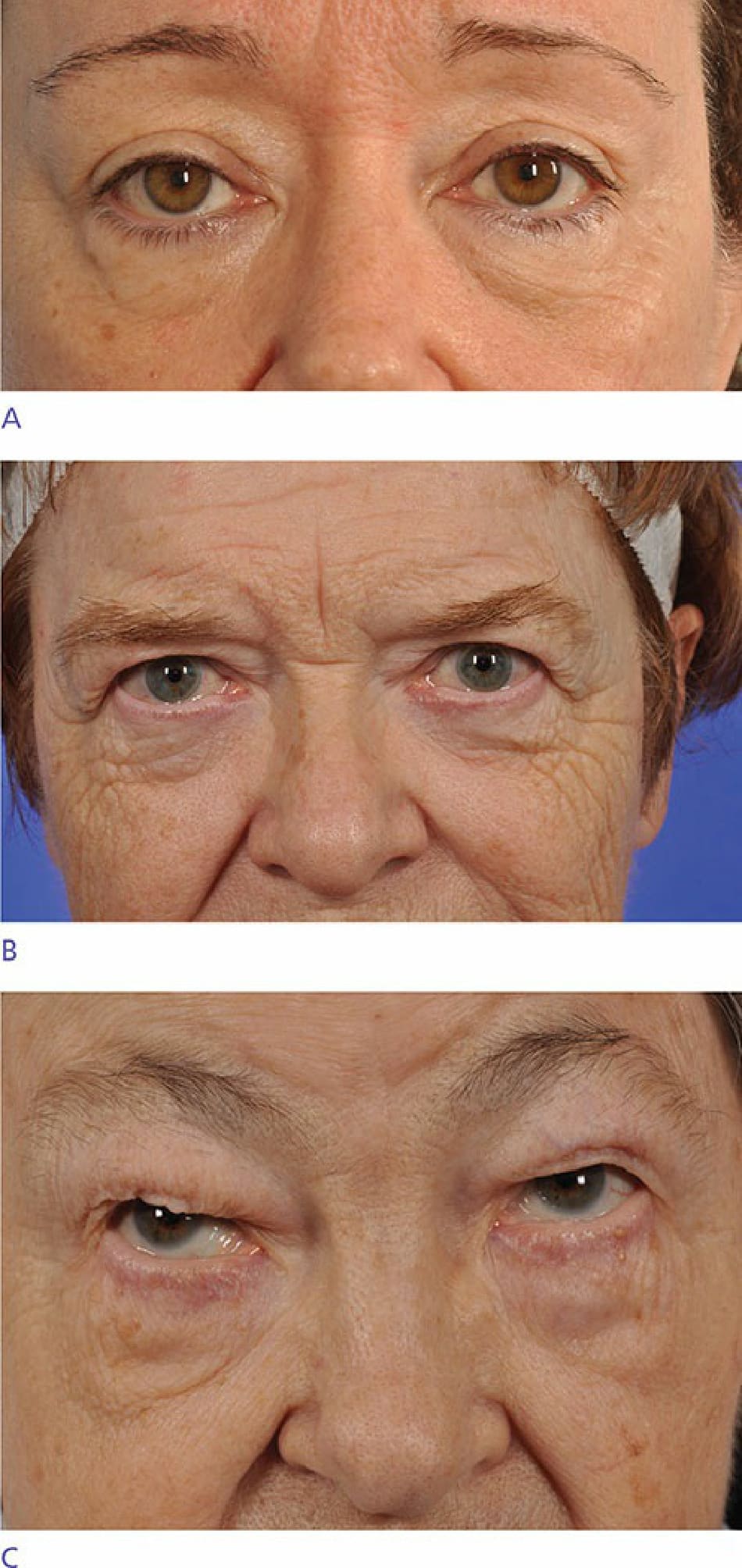
Figure 73-14. Mild (A), moderate (B), and severe (C) degrees of upper eyelid fat prolapse.
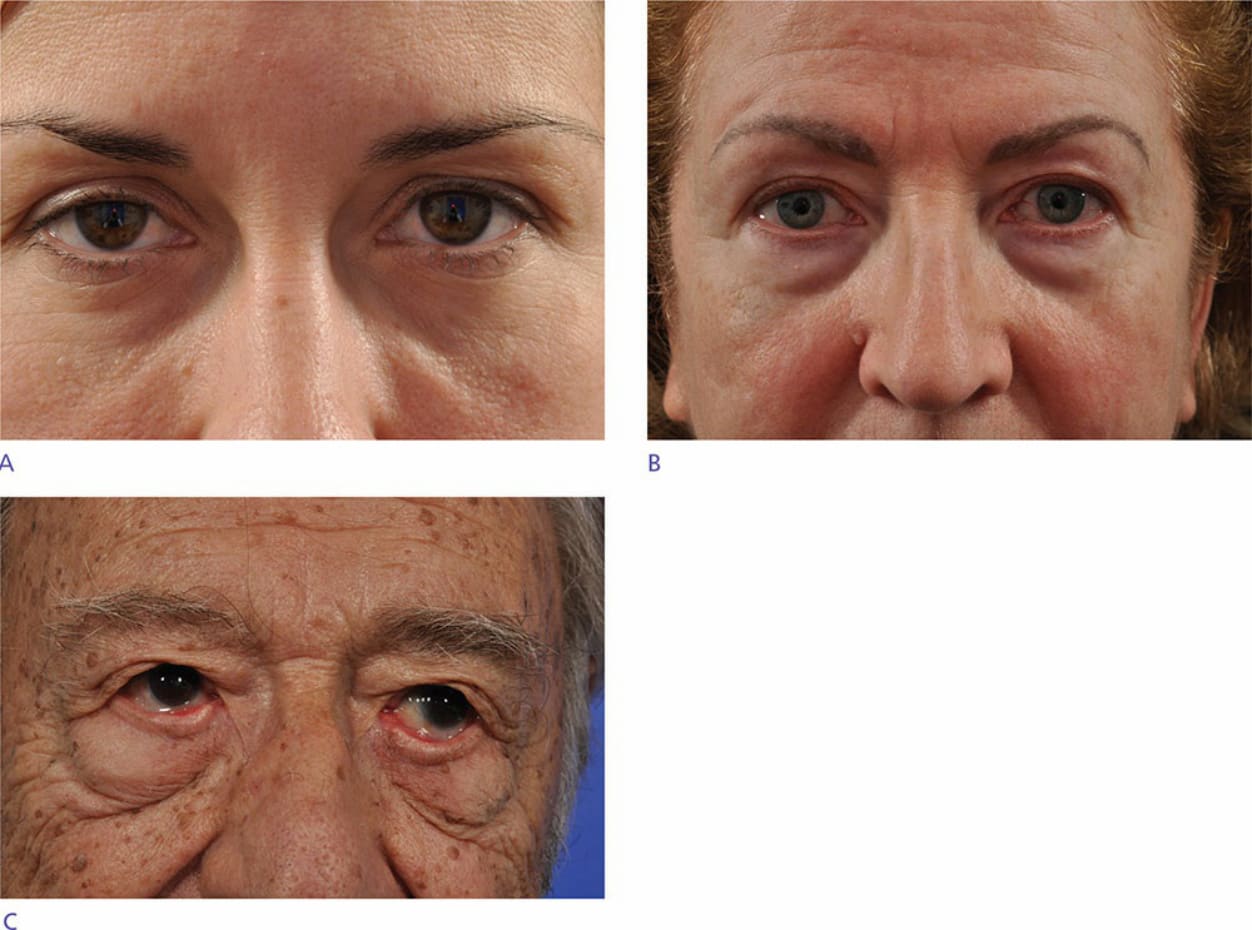
Figure 73-15. Mild (A), moderate (B), and severe (C) degrees of lower eyelid fat prolapse.

Figure 73-16. Negative eyelid vector. Note that the anterior surface of the cornea extends beyond the lower lid border.
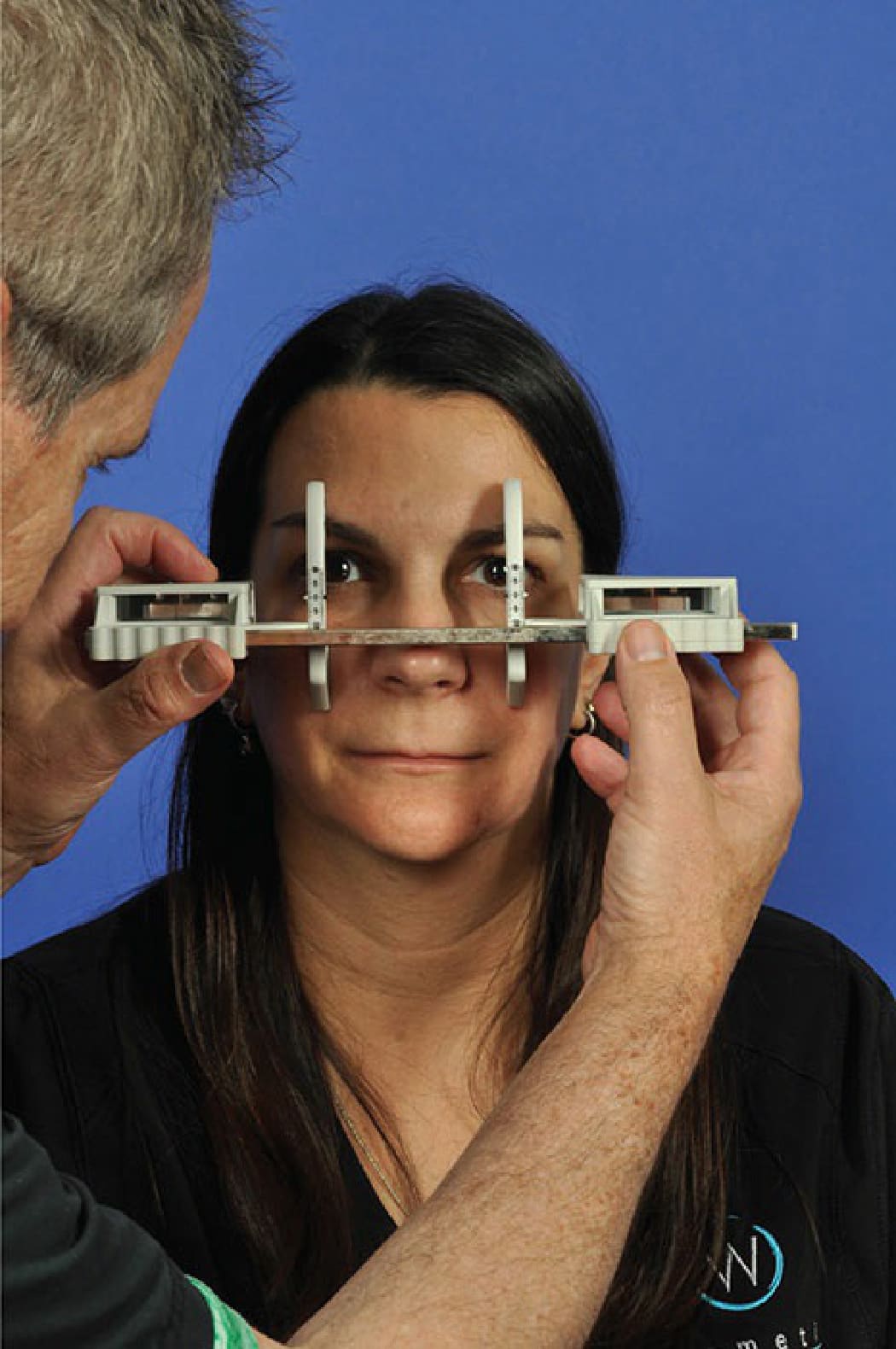
Figure 73-17. Hertel exophthalmometry testing.
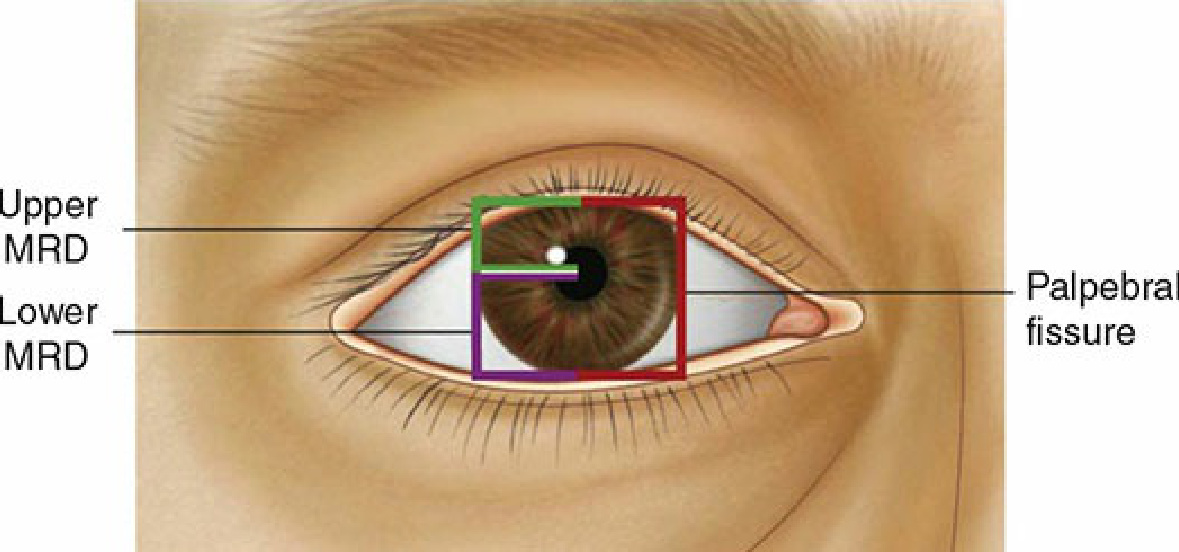
Figure 73-18. Ptosis is defined as a marginal reflex distance (MRD) less than 2 mm as measured from the pupil center to the upper lid margin. (Reproduced with permission from Robinson JK, Hanke CW, Siegel DM, et al: Surgery of the Skin, 3rd edition. Philadelphia: Elsevier, Inc; 2015).

Figure 73-19. Snap back testing of the lower eyelid.