ANATOMY
ANATOMY
A strong grasp of periorbital anatomy is important in order to execute an appropriate surgical plan for patients undergoing eyelid surgery. The upper eyelid, moving from superficial to deep, is comprised of skin and orbicularis oculi muscle. The orbicularis muscle is the main protractor, or closer, of the eyelid and has three different functional segments (Fig. 73-6). The pretarsal and preseptal orbicularis muscles (referred to as palpebral orbicularis as a unit) allow for involuntary blinking. The pretarsal orbicularis muscle originates from the posterior lacrimal crest and the anterior limb of the medial canthal tendon. The preseptal portion of the muscle originates from the upper and lower borders of the medial canthal tendon.4 Sparing of these structures during upper eyelid blepharoplasty may reduce postoperative complications such as dry eye and poor lid closure, as well as preserve fullness to the upper lid.5,6 The orbital orbicularis muscle encircles the orbital rim and originates from the medial canthal tendon, frontal process of the maxilla, and the orbital process of the frontal bone.7 Orbital orbicularis muscle is responsible for forced eyelid closure.
Posterior to the pretarsal orbicularis lies the tarsus, which is 8 to 10 mm in height in the upper lid and 3 to 4 mm in the lower lid (Fig. 73-7). Superior to the tarsus and deep to the orbicularis muscle is the orbital septum, which is a fibrous, avascular structure that originates from the periosteum of the superior orbital rim (arcus marginalis) and inserts onto the superior aspect of tarsus. This structure delineates the pre- and postseptal spaces of the eyelid and orbit.
Beneath the orbital septum are the nasal and central upper eyelid fat pads, as well as the orbital lobe of the lacrimal gland laterally. The central fat pad is also referred to as the preaponeurotic fat compartment. In addition to their location, these two fat compartments can be distinguished by their color; the nasal pad is pale yellow or white while the central fat pad is more yellow.8 With aging, the nasal fat pad is most likely to become visible through attenuated septum,8 and it can be debulked at the time of blepharoplasty surgery. More recently, the tendency has shifted to preservation of upper eyelid fat, especially with regard to the central compartment where fat can be mobilized and preserved.9
The lacrimal gland occupies the most lateral postseptal compartment in the upper eyelid. Composed of a larger orbital lobe and a smaller palpebral lobe, it resides in a fossa of the frontal bone in the superotemporal orbit (Fig. 73-8). The palpebral lobe is often visible with eversion of the upper eyelid. However, with age, it is the orbital lobe that may prolapse anteriorly and manifest as a fullness in the lateral upper eyelid (Fig. 73-9). Other, noncompartmentalized fat may also contribute to lid fullness in the aging face, especially among Asians.10
Deep to the upper eyelid fat compartment is the levator palpebrae superioris muscle. It arises from the periorbita of the lesser wing of the sphenoid bone at the orbital apex, just outside the Annulus of Zinn. As the levator muscle extends anteriorly within the orbit, it transitions to become an aponeurosis at Whitnall’s ligament and sharply changes to a more inferior direction. It then divides into an anterior and posterior portion within the eyelid. The posterior portion inserts on the anterior aspect of tarsus, while the anterior portion projects to pretarsal orbicularis muscle and skin, contributing to the formation of the upper eyelid, or pretarsal, crease.
The position of the lid crease varies with gender, ethnicity, and age. In Caucasians, the upper eyelid crease is usually found 8 to 9 mm above the superior lash line in men and 9 to 11 mm above the lash line in women.11 In Asians, the lid crease may be absent or very low because of a more inferior insertion of septum and/or absent insertion of the levator aponeurosis into the dermis.12–14 The lid crease may be higher or absent in patients with aponeurotic or congenital ptosis. Muller’s muscle originates on the undersurface of the levator muscle and inserts on the superior margin of tarsus. Both the levator and Muller’s muscles function as eyelid retractors, and are separated from each other by the rich vascular plexus of the peripheral arterial arcade.
Since the eyebrow and upper eyelid are often considered as a continuum, the position of the brow is of vital component in the assessment of the upper eyelid.15 In general, the highest peak of the brow is at the central and lateral junction, corresponding to the lateral corneal limbus. In women, a youthful brow resides 0.5 to 1 cm above the
superior orbital rim. In men, the youthful brow position is lower, residing at or slightly above the orbital rim, and the brow contour is more flat and less arched.16 Depending on the degree of sub-brow fat atrophy, aging patients may present with significant lateral hooding in addition to dermatochalasis.
In many ways, lower eyelid anatomy is similar to the anatomy of the upper eyelid, with a few important differences. Moving from superficial to deep, thin skin is found above the palpebral and orbital components of orbicularis oculi muscle, and the septum underlies the muscle. The lower lid retractors are less distinct than those in the upper lid and are comprised of (a) the capsulopalpebral fascia, which originates from terminal fibers of the inferior rectus muscle, and (b) the inferior tarsal muscle, which originates from the posterior aspect of the capsulopalpebral fascia. The capsulopalpebral fascia and inferior tarsal muscle are analogous to the levator aponeurosis and Muller’s muscle (otherwise known as the superior tarsal muscle), respectively. After fusing with the orbital septum, which originates from the periosteum of the infraorbital rim at the arcus marginalis, the lower lid retractors insert on the inferior margin of tarsus.
Three fat compartments are found in the lower eyelid, rather than two, as are found in the upper eyelid (Fi g. 73-7). The medial, central, and lateral fat pads reside posterior to the orbital septum. The inferior oblique muscle is found between the medial and central fat pads, while an extension of Lockwood’s ligament, the suspensory ligament of the lower eyelid, is found between the central and lateral fat pads.17 In youth, the orbital septum and Lockwood’s suspensory ligament have strong tone, maintaining the fat pads posterior to a vertical vector connecting the lid margin to the orbital rim. The configuration of the palpebral fissure is maintained by the medial and lateral canthal tendons, which are a blending of attachments from the orbicularis muscle and tarsus that fuse onto orbital periosteum. Tightening of the lateral canthal tendon may be performed at the time of lower lid blepharoplasty to reduce the likelihood of postsurgical ectropion.
Unique to the lower lid are the orbital retaining ligament and the tear trough. The orbital retaining ligament (also referred to as the orbitomalar ligament)18 originates from the arcus marginalis as a condensation of connective tissue that divides the orbital orbicularis from the preseptal orbicularis and attaches to the dermis. This multilaminate ligament suspends the malar fat pad.19–21 The tear trough is a dense attachment of the orbicularis to the anterior maxillary crest seen medial to the mid-pupillary line. Also known as the nasojugal fold, this concavity is relatively devoid of suborbicularis fat. Immediately inferior to the tear trough are the attachments of the levator labii superioris and the levator alequae nasae.20
The ligament and/or its attachments to skin may attenuate over time and give rise to descent of the malar fat pad. Ptosis of the malar fat pad gives rise to both the so-called
concavity convexity deformity at the lid cheek junction (palpebromalar groove) and to the apparent lower eyelid lengthening seen with aging.22 The concavity seen in aging represents an area of soft-tissue deficit between the relative convexities of the pseudoherniated fat of the lower eyelid and the ptotic malar fat pad.
Descent of the midface gives rise to the inverted V deformity, as the aged ptotic and atrophic malar fat pad appears suspended to the orbital rim and hangs from the tear trough. The V deformity is thought to arise as a result of several descending forces in the lower lid and midface. First, there is stretching of the superficial muscular aponeurotic system (SMAS) in the lateral midface, allowing the malar fat and suborbicularis oculi fat (SOOF) to descend inferiorly. Second, the nasojugal fold medially deepens and becomes more pronounced. These two medial and lateral forces contribute to the appearance of an inverted V-shaped deformity in the lower lid.
Elastic and smooth skin contributes to a youthful eyelid appearance. Important skin changes of the aging eyelid include thinning, loss of elasticity, hyperpigmentation, and actinic changes, as well as increased laxity of the orbicularis muscle and canthal tendons.22,23 Changes in orbicularis muscle tone and decreased skin elasticity may contribute to the increased lower eyelid length commonly seen in the aging face.24 Bone structure also changes with age, and atrophy of the orbital rim may contribute to the apparent changes related to volume loss in the aging face.25
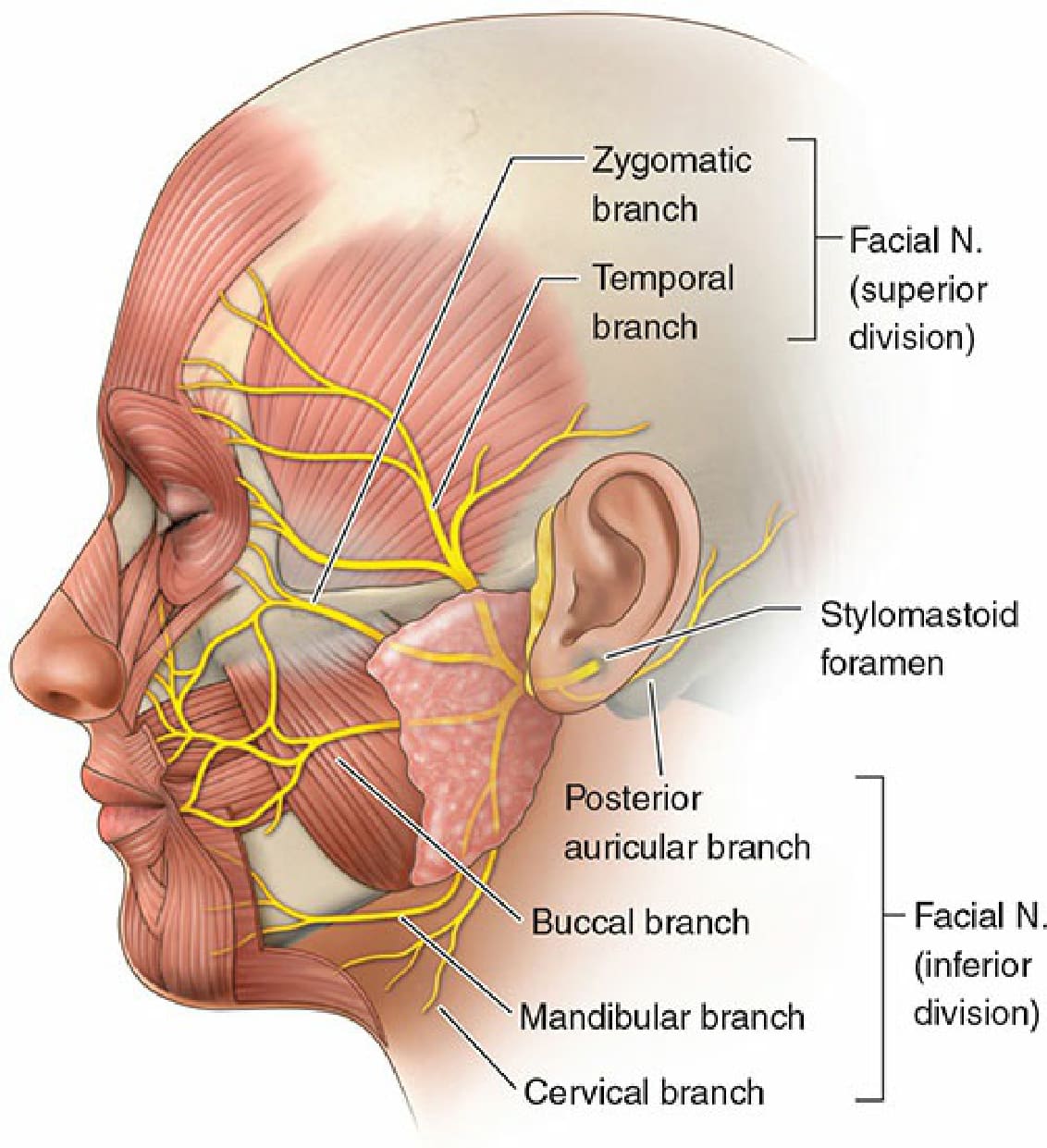
Figure 73-6. The facial nerve innervates the orbicularis oculi muscle.
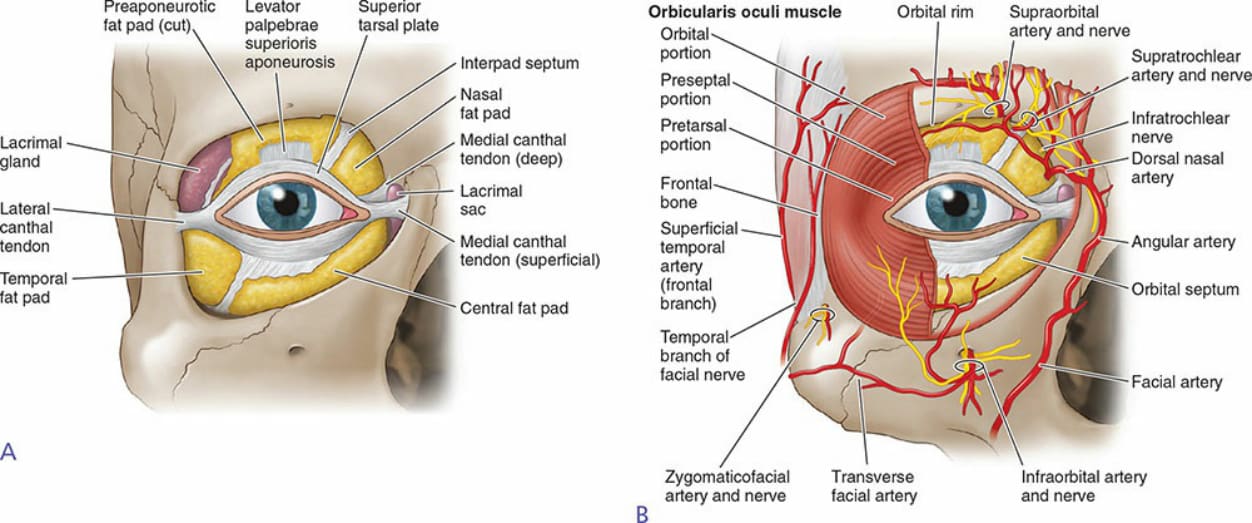
Figure 73-7. Eyelid anatomy.
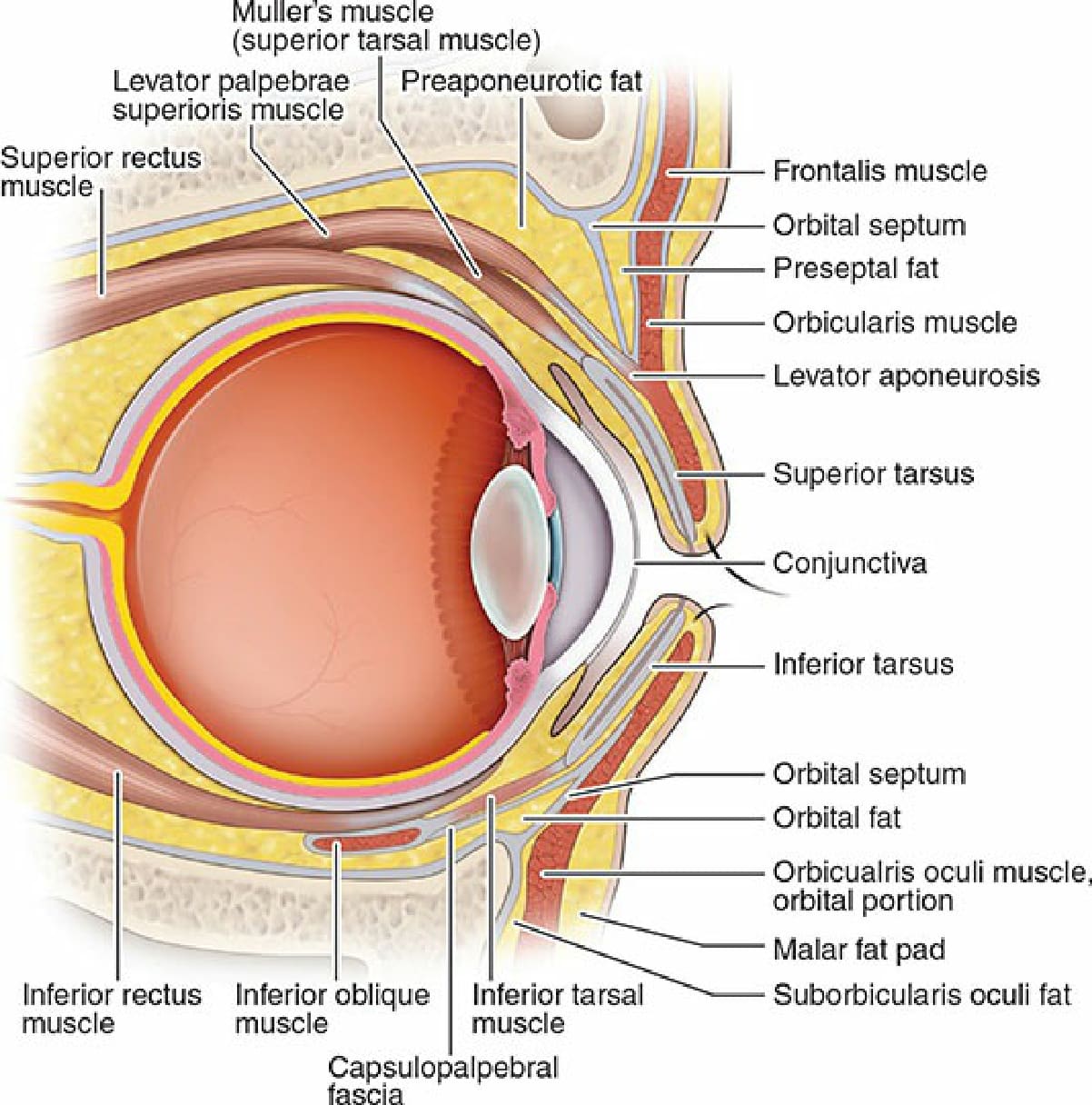
Figure 73-8. Upper and lower eyelid structures.

Figure 73-9. Unilateral lacrimal gland prolapse.