Introduction
CHAPTER 73 Blepharoplasty
Karen E. Revere Allan E. Wulc
SUMMARY
Blepharoplasty is the most frequently performed facial aesthetic surgical
procedure in the United States.
Blepharoplasty is primarily used to treat dermatochalasis, and both upper and
lower blepharoplasty result in a more alert and youthful appearance.
Anesthesia options include local anesthesia, local anesthesia with IV sedation,
and general anesthesia.
Beginner Tips
Be sure to distinguish between eyelid ptosis, brow ptosis, and dermatochalasis.
Upper lid blepharoplasty with en bloc excision of upper lid skin, orbicularis oculi
muscle, and/or orbital fat is the gold standard for the correction of dermatochalasis.
The consequences of aggressive skin removal are more difficult to correct than the
consequences of managing residual skin excess.
Expert Tips
Superior sulcus hollowing is a common postoperative complication, prompting a
recent shift toward volume preservation in upper lid blepharoplasty.
Lid malposition seems to occur less frequently with concomitant canthal suspension.
Instead of fat excision, many now advocate for fat preservation and repositioning as a
more effective means of lower lid and mid-face rejuvenation.
Don’t Forget!
Negative-vector patients (those with prominent eyes without bony support) are at
increased risk of ectropion and dry eye postoperatively.
There is significant variation in technique options, though what the surgeon knows and
is most comfortable with might be more important that the actual choice of technique and surgical approach.
Pitfalls and Cautions
Brow ptosis should be distinguished from dermatochalasis. If both problems are
present and blepharoplasty alone is performed, the degree of brow ptosis may be worsened.
With transcutaneous lower eyelid blepharoplasty, lower eyelid ectropion and
retraction can occur in up to 30% of cases.
For lower eyelid blepharoplasty, avoid excessive skin removal; usually only 2 mm of
skin excision is required at the most.
Patient Education Points
Controlling patient expectations is critical.
If the patient does not want brow surgery, they should be made aware that the degree of
brow ptosis could worsen after isolated blepharoplasty, creating the appearance of excess upper lid skin from the descended brow.
Counsel patients that the need for additional skin removal should not adversely
influence an overall successful cosmetic outcome.
Billing Pearls
Most insurance companies require clinical photographs and visual field images for
preapproval purposes.
Aesthetic blepharoplasty patients may benefit from combining blepharoplasty with
other procedures, and sometimes they can see cost savings by doing this.
CHAPTER 73 Blepharoplasty
INTRODUCTION
Blepharoplasty is the most common aesthetic surgical procedure performed on the face in the United States,1 and its goal is to restore a youthful contour to the eyelids and midface. Upper and lower eyelid blepharoplasty are two distinct procedures with distinct aesthetic aims. Upper blepharoplasty is performed to address excess skin, asymmetric eyelid creases, fat or lacrimal gland prolapse, and/or sulcus hollowing. Lower blepharoplasty is performed to address the orbitomalar region, including teartrough deformity and/or prominence of the lid–cheek junction. While an excellent cosmetic outcome is always attempted, patients may seek blepharoplasty surgery for functional, cosmetic, or a combination of reasons.
The most commonly used word for excess eyelid skin is dermatochalasis, which refers to the fine wrinkling and loosening of eyelid skin that occurs with age (Fig. 73-1). Blepharochalasis is another frequently used term, though it more accurately refers to a syndrome of cyclic eyelid edema that usually occurs in younger patients (Fig. 73-2). Blepharochalasis can lead to thinning of eyelid skin, atrophy or prominence of the eyelid fat pads (depending on the phase of the condition), ptosis, and increased eyelid laxity.2 Steatoblepharon is commonly associated with dermatochalasis, and describes prominent upper and/or lower eyelid fat pads (Fig. 73-3). It is important to distinguish between dermatochalasis, eyelid ptosis, and brow ptosis. Upper eyelid ptosis occurs when the eyelid falls lower than its normal position, which is usually 2 to 3 mm above the superior corneal limbus in central gaze (Fig. 73-4).3 When the brow falls below the level of the superior orbital rim, a diagnosis of brow ptosis is made (Fig. 73-5). This may accentuate the appearance of dermatochalasis, and can be addressed simultaneously with upper blepharoplasty.

Figure 73-1. Bilateral upper eyelid dermatochalasis.

Figure 73-2. Bilateral blepharochalasis.

Figure 73-3. Bilateral steatoblepharon.

Figure 73-4. Right upper eyelid ptosis.
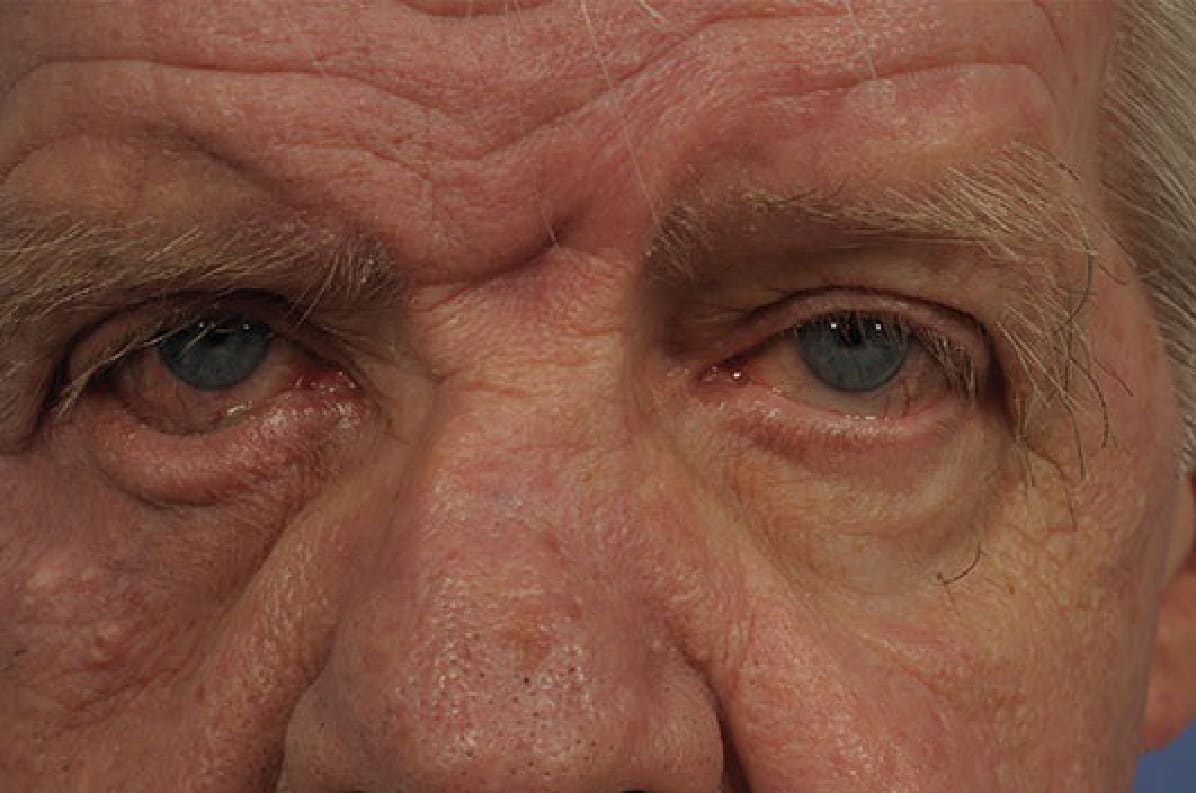
Figure 73-5. Bilateral brow ptosis and right lower eyelid ectropion.