ANATOMICAL CONSIDERATIONS
ANATOMICAL CONSIDERATIONS
Intimate knowledge of the venous system and interconnections between the veins is a prerequisite prior to performing sclerotherapy. The axial veins of the venous system of the lower extremity are divided into the superficial and deep systems. Veins that traverse the same system are termed communicating veins, whereas veins that connect the superficial to the deep system are called perforating veins. The superficial veins are contained in the subcutaneous tissue of the lower extremity within a superficial space that is bounded deeply by the muscular fascia and superficially by the dermis. The major axial superficial veins of the lower extremity include the great and small saphenous veins. Other lower extremity superficial veins with more variant anatomy include the anterior, posterior, and superficial accessories of the great saphenous vein (GSV), the superficial accessory of the small saphenous vein, intersaphenous veins, and the lateral venous system (Fig. 72-2).
The deep veins of the lower extremity are contained within the deep muscle
compartments bounded by the muscle fascia (Fig. 72-3). The deep veins of the lower extremity are classified as intramuscular (within a single muscle) or intermuscular (between muscle groups). The intermuscular veins are more important in the development of chronic venous disease. Sclerotherapy is effective in destroying a segment or length of vein that is usually axially oriented, though it cannot safely and predictably eradicate a circumferential finite point of reflux, such as a junction at which two veins converge, without the potential risk of concomitantly obliterating some length of vein distal and proximal to this point of reflux. As an example, injection of a sclerosant at the point of an incompetent saphenofemoral junction could produce destruction of the adjacent segments of the femoral vein and the greater saphenous vein. Injection of a sclerosant seldom obliterates incompetent perforating veins, but merely the varicosity of the superficial venous system into which these perforating veins empty. It is advised that all sites of reflux from the deep venous system into the superficial varicosities should be surgically treated before sclerotherapy, as this would diminish the development of new varicosities by preventing retrograde flow, as well as associated elevated venous pressure, into adjacent competent veins. It also aids in minimizing retrograde flow into existing varicosities that are the targets of treatment.34
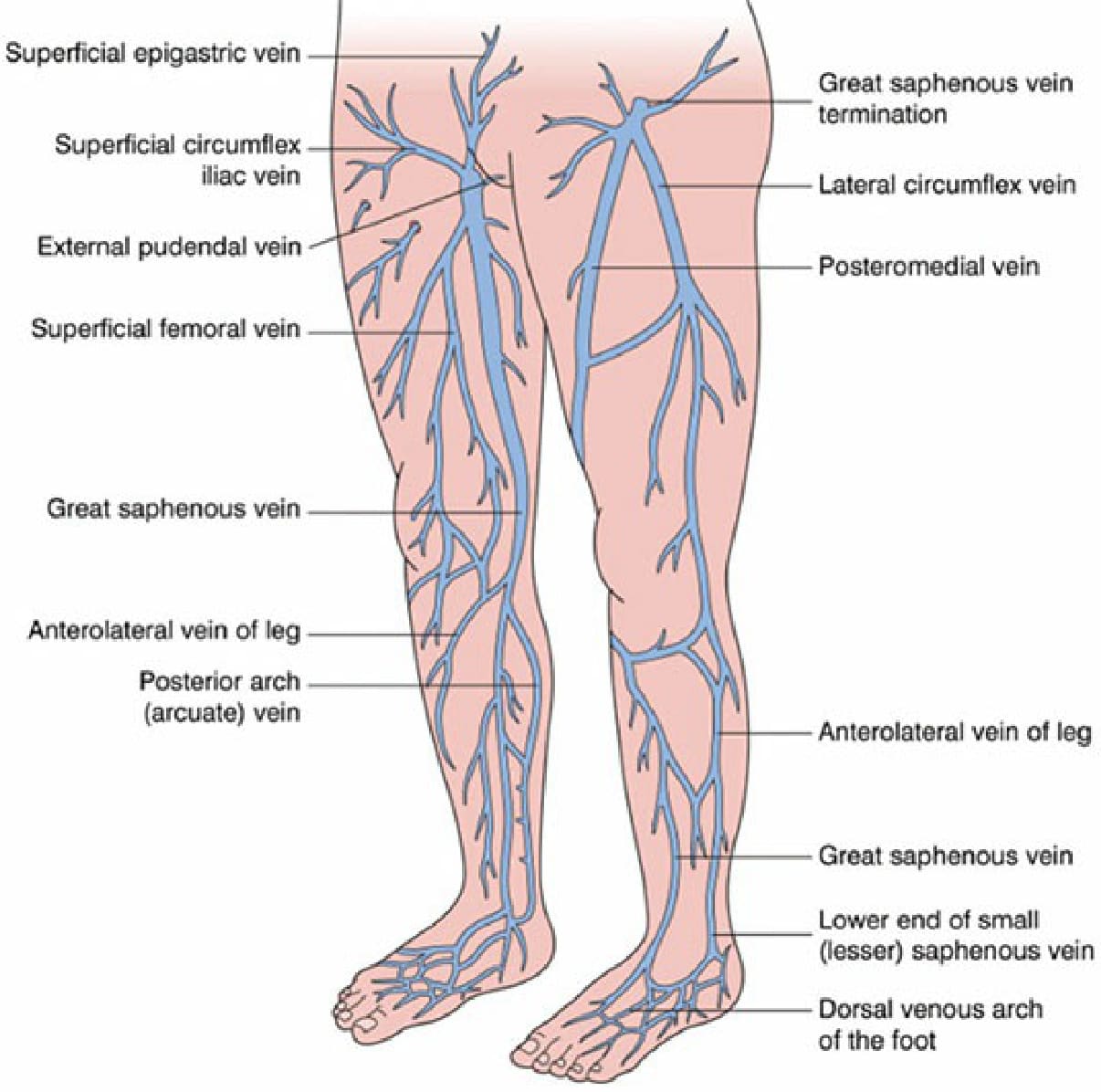
Figure 72-2. Superficial veins of the lower extremity. (Reproduced with permission from Bolognia JL, Jorizzo JL, Rapini RP: Dermatology, 2e. Philadelphia: Elsevier, Inc.; 2008)
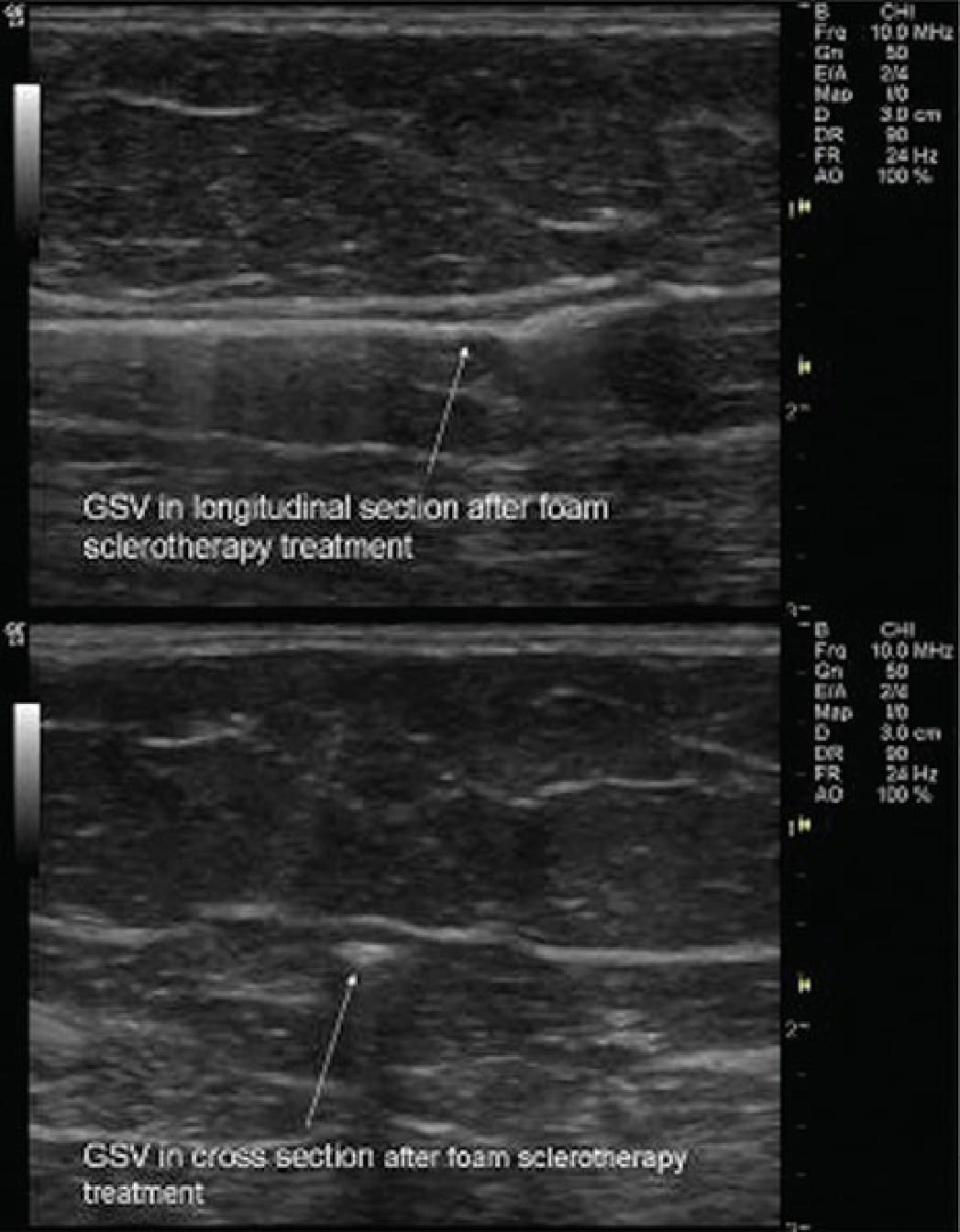
Figure 72-3. Cross and longitudinal sections from ultrasound-guided foam sclerotherapy (UGFS) after treatment of great saphenous vein.