Leg veins
Leg veins
Visible leg veins, composed of telangiectasias and venulectasias occur in approximately 80% of adults in the United States. Leg veins are caused by venous valvular incompetence resulting in increased hydrostatic pressure and vessel dilation. They most commonly occur on the legs due to gravitational dependency. Candidates for leg vein laser treatment include those with a prior history of minimal response to sclerotherapy, adverse reaction to sclerosing agents, telangiectatic matting, ankle veins, and needle phobias.23
Both KTP and PDL have been used for the treatment of leg veins. These lasers are limited by their depth of penetration, resulting in significant inconsistency in treatment outcomes. Primary complications include hyper- and hypopigmentation, which has been reported to occur in 20% to 40% of patients.8 Broadband IPL has been used to treat leg veins with single, double, and triple pulsing with limited success, though cutoff filters may increase its efficacy. There is a relatively high incidence of dyspigmentation, possibly due to nonspecific chromophore selection. Longer wavelength lasers such as the long-pulsed Alexandrite and long-pulsed diode have been tried with pulse durations ranging from 3 to 20 ms and 5 to 20 ms, respectively. There have been some encouraging reports,24,25 though the results have been inconsistent (Fig. 64-5).
Long-pulsed Nd:Yag lasers with gel cooling have been used with fluences up to 150 J/cm2, pulse duration 1 to 15 ms (single, double, triple pulsing can be applied), and a spot size of 6 mm. The treatments can be repeated at 6- to 8-week intervals. Caution must be taken with multiple passes, which can result in vessel rupture with subsequent hemosiderin deposition. The advantages of long-pulsed Nd:Yag lasers include adequate depth of penetration, minimal melanin absorption, and the ability to treat a full range of leg veins (up to 3 mm diameter and 5 mm depth) in darker and lighter skin types.
Laser approaches provide a noninvasive alternative to needle therapy or microphlebectomy. Complications may include scarring and pigment alteration primarily due to hemosiderin deposition. A combination of lasers, phlebectomy, and sclerotherapy may be the best long-term approach for treating leg veins.26 As a monotherapy, sclerotherapy remains the gold standard treatment for leg veins.
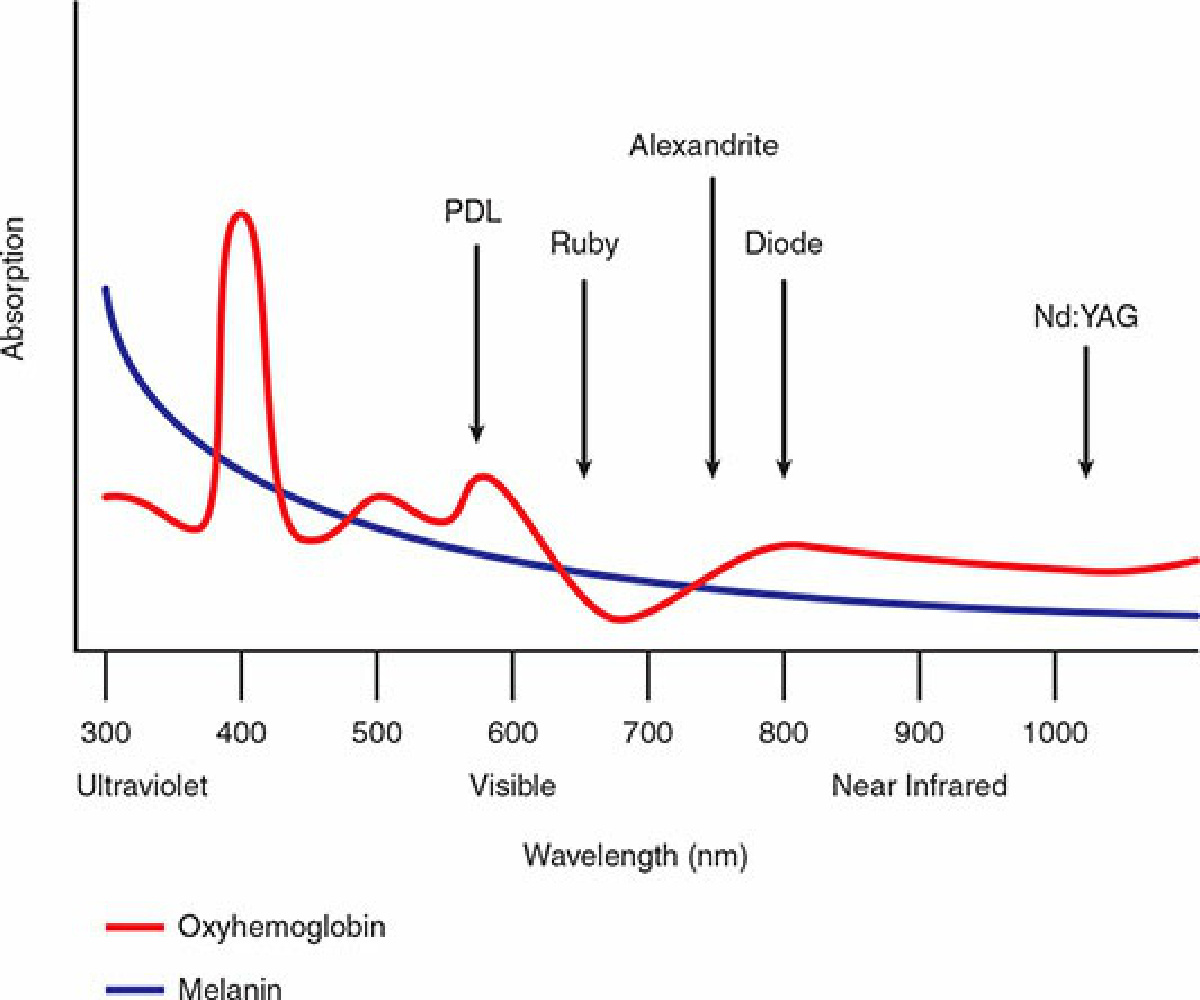
Figure 64-5. When choosing the appropriate laser for vascular lesions, the different absorption spectra for hemoglobin and melanin should be considered.