Patient preparation
Patient preparation
Starting 2 weeks prior to the procedure, the patient is advised to abstain from all medications and supplements that may increase the risk of bruising or bleeding.
The day before fat grafting, the patient is advised to start cephalexin 500 mg twice daily, or ciprofloxacin 500 mg twice a day, and to continue for a total of 7 days.
Valacyclovir is prescribed starting 1 day before the procedure if facial fat grafting is to be performed.
Preoperative medication The patient’s weight, measurements, photographs, markings, and vital signs are taken prior to administering preoperative medication. For large fat transfer procedures, a mild sedative, such as diazepam 10 mg, is administered at least 30 minutes prior to the start of the procedure. If desired, an oral narcotic such as Lortab, which contains 10 mg of hydrocodone and 650 mg of acetaminophen, may also be administered. Prednisone 40 mg may also be administered orally if facial fat grafting is to be performed.
Patient marking of the body and face Body areas for liposuction and fat transfer are marked with sterile surgical pens and permanent markers while the patient is standing in front of a mirror in the examination room. Areas of excess fat, depressions, the midline, and bony landmarks are carefully marked topographically with different colors, typically red for depressions, green or blue for excess fat, and black for bony landmarks. On the face, the areas for fat grafting, bony landmarks, location of the marginal mandibular nerve, and cannula entry sites are marked with the patient sitting upright in front of a mirror in the exam room. It is important that all detailed topographical markings are made prior to infusing any local anesthesia or tumescent solution, because the tumescence can obscure the soft tissue and bony landmarks of the face and body.
Patient preparation in the operating room After the treatment areas are marked, the patient is brought to the operating room, prepped with chlorhexidine, and draped and positioned in a sterile fashion. An intravenous line may be inserted prior to the liposuction procedure. The patient may be connected to a cardiac monitor with continuous heart rate, blood pressures, EKG, and pulse oximetry throughout the fat harvesting and grafting procedure. If desired, an ultrasound system may be present in the operating room with a sterile sleeve attached to the transducer so that it can be utilized for ultrasonic guidance during the fat grafting procedure.
Before starting the fat grafting procedure, the recipient areas for fat grafting are reprepped and new sterile drapes, gowns, and gloves are used.
Tumescent anesthesia by infusion pump Tumescent infusion of the donor sites is performed with a blunt cannula in the same manner as when performing liposuction alone. After local anesthesia at the marked entry port is obtained, an incision is made with a 2.5- to 3.0-mm dermal punch or a #15 scalpel. Then a blunt 1.5-mm infiltration cannula is carefully inserted superficially parallel to the skin surface so that the outline of the cannula remains visible beneath the skin surface and the tip of the cannula can be felt and monitored by the opposite hand, the “smart hand,” at all times during the infusion. The infiltration cannula is used to slowly infuse a small amount of tumescent solution into the superficial subcutaneous fat in the treatment area in a radial pattern, using an infusion pump. Infrasonic vibration handpieces may make the infusion phase more comfortable for the patient.
Tumescent anesthesia by syringe For small donor sites, local tumescent anesthesia can be obtained manually via syringe. After a small bleb of local anesthesia is injected at the marked entry port, an incision is made with a 2.5-mm dermal punch or a #15 scalpel. A 22-gauge spinal needle or a 1.2- mm infiltrating cannula attached to a 10-cc syringe is carefully inserted superficially through the entry port, parallel to the skin surface. The area is then carefully infused beginning in the subdermal plane in a radial pattern, gradually extending into the deeper layers of the subcutaneous fat while remaining above the fascia, until the entire elliptical area of the donor site is tumesced.
Waiting period after tumescence A 20-minute waiting period after the completion of tumescent infusion is recommended to permit vasoconstriction from the epinephrine to take effect.
During this waiting period, external ultrasound or vibratory massage can be performed on the donor sites prior to initiating liposuction to initiate a gentle fat emulsification.
Fat harvesting by machine liposuction There are many options available for fat harvesting and fat extraction. Most methods are chosen based on improved fat survival and personal preference. Fat can be harvested by performing liposuction by hand with a syringe or by performing liposuction with a vacuum pump and an ultrasonic, infrasonic, or power-assisted device. Laser devices are not used for fat harvesting, as few viable fat cells are present in the aspirate after laser liposuction.
Many systems are used for machine harvesting, including the Power X rotational power-assisted device (Solta Medical); the ultrasonic Vaserlipo fat emulsion device (Solta Medical); and the infrasonic nutational Tickle Lipo fat emulsion device (Euromi). Liposuction for fat harvesting is typically performed in the same manner as liposuction
for body contouring, with a few exceptions. A lower vacuum pressure is recommended for aspiration and specialized harvesting cannula such as the Mendieta with the Power X and Rubelo or Viterbo on the Tickle Lipo are often utilized (Figs. 61-1 to 61-4).
Fat harvesting by syringe When harvesting modest amounts of fat, manual syringe harvesting may be performed.
- Connect a Coleman harvesting cannula to a 10-cc syringe.
- Insert the cannula through the entry port into the middle depth of the excess
subcutaneous tissue at the donor site.
3. After insertion, pull the barrel of the syringe back about 1 to 2 cc to maintain
continuous suction while making several back and forth motions in a radial pattern at the donor site in order to harvest the fat.
4. When the syringe is full of fat aspirate, cap it, and place it vertically in the syringe
stand.
5. Allow the syringes to stand for several minutes to allow gravity separation to take
place.
Fat collection and separation Many different fat collection and processing methods and systems exist for separating the viable fat cells from the lipoaspirate fluid that contains tumescent fluid, blood, and lipids. These include special collection systems, fat collection bottles, special filter systems, manual gravity separation, gravity separation with centrifugation, and external straining. After initial decanting, antibiotics and platelet-rich plasma (PRP) may be added to the separated fat prior to additional gravity separation (Figs. 61-5 and 61-6).
Fat extraction from vacuum pump lipoaspirate A. Gravity separation method: a. First gravity separation: Decantation of serous fluid after gravity separation from
sterile container with or without a sterile filter trap. b. Second gravity separation: Gravity-separated fat is withdrawn into separate 60-cc
Toomey syringes. Each capped syringe is placed vertically in a syringe rack. After 10 to 30 minutes, the serous fluid is decanted from the Toomey syringes. c. Centrifuged separation: May be performed but may damage the fragile fat cells. d. After separation, the fat for grafting is transferred to large 60-cc Toomey syringes if
large areas such as the breasts and buttocks are to be grafted. If facial fat augmentation is planned, a Toomey to Luer lock adaptor is utilized to transfer the fat to individual 1-cc Luer lock syringes. These 1-cc syringes are placed vertically in a small syringe rack (Figs. 61-7 to 61-17).

Figure 61-1. A vacuum pump and the Power X rotational power-assisted device and the ultrasonic Vaser system can each be used alone or together to harvest fat for fat grafting.

Figure 61-2. The infrasonic nutational Tickle Lipo device by Euromi can be used to tumesce, emulsify, and harvest fat for grafting.

Figure 61-3. The infrasonic vibration of the Tickle Lipo nutational handpiece (Euromi) can increase patient comfort during infusion because of the gateway theory of nerve conduction of pain.

Figure 61-4. The Tickle Lipo nutational handpiece (Euromi) with aspiration cannula uses infrasonic energy to emulsify fat while aspirating fat, providing a more comfortable experience for the patient while producing a lipoaspirate that is rich in viable adipocytes.
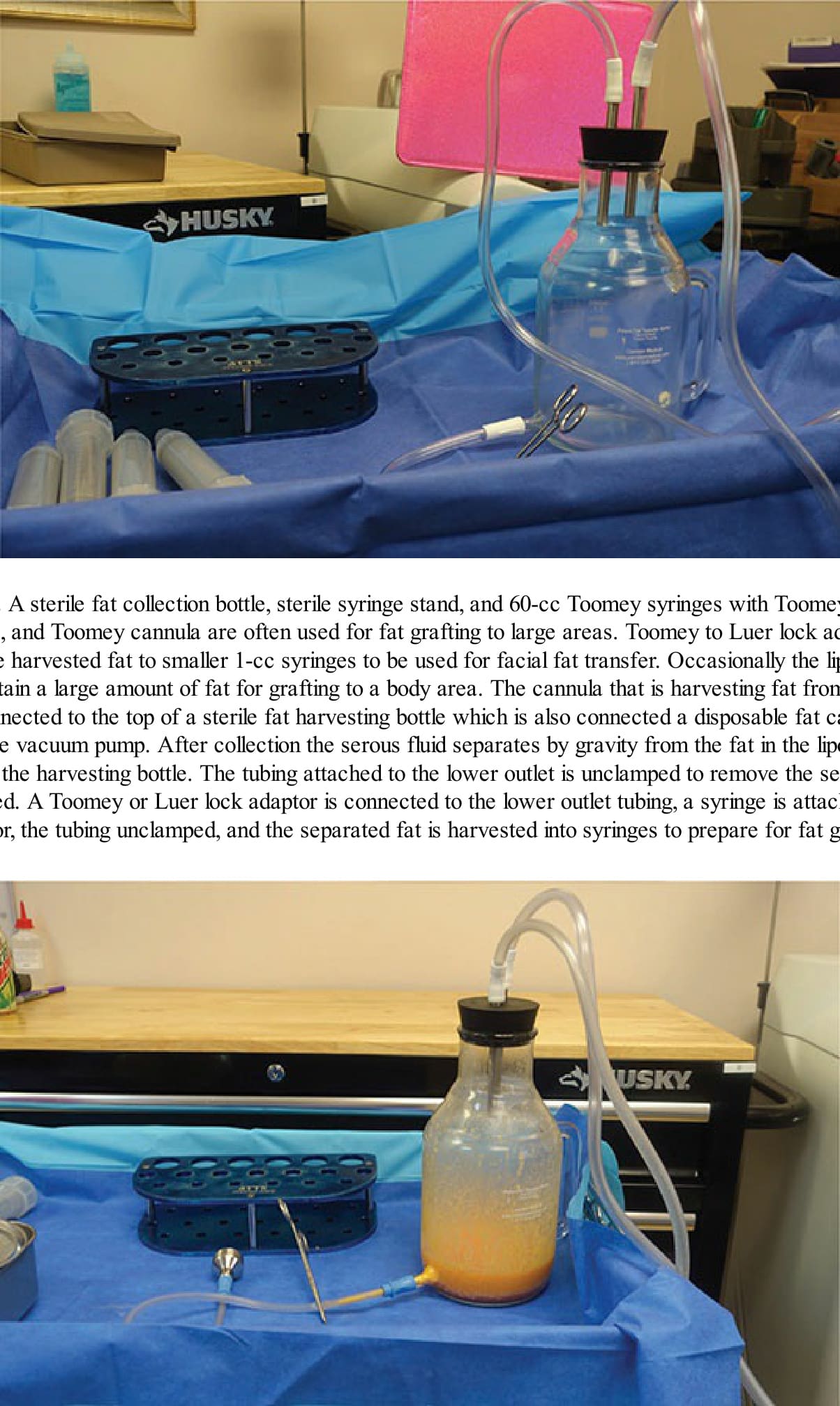
Figure 61-5. A sterile fat collection bottle, sterile syringe stand, and 60-cc Toomey syringes with Toomey adaptors, Toomey plugs, and Toomey cannula are often used for fat grafting to large areas. Toomey to Luer lock adaptors permit transfer of the harvested fat to smaller 1-cc syringes to be used for facial fat transfer. Occasionally the lipoaspirate is strained to obtain a large amount of fat for grafting to a body area. The cannula that is harvesting fat from the patient is directly connected to the top of a sterile fat harvesting bottle which is also connected a disposable fat canister attached to the vacuum pump. After collection the serous fluid separates by gravity from the fat in the lipoaspirate to the bottom of the harvesting bottle. The tubing attached to the lower outlet is unclamped to remove the serous fluid, then reclamped. A Toomey or Luer lock adaptor is connected to the lower outlet tubing, a syringe is attached to the special adaptor, the tubing unclamped, and the separated fat is harvested into syringes to prepare for fat grafting.

Figure 61-6. Sterile fat collection bottle in the process of filling.

Figure 61-7. A Toomey adaptor is connected to the lower outlet tubing to prepare for placement in 60-mL Toomey syringes, which are often preferred for body fat grafting because they tend to clog less than Luer syringes.

Figure 61-8. A Toomey syringe is attached to the Toomey adaptor, the tubing unclamped, and the separated fat is harvested into 60-mL syringes to prepare for fat grafting. Harvested fat can also be transferred to Luer lock syringes of different sizes.
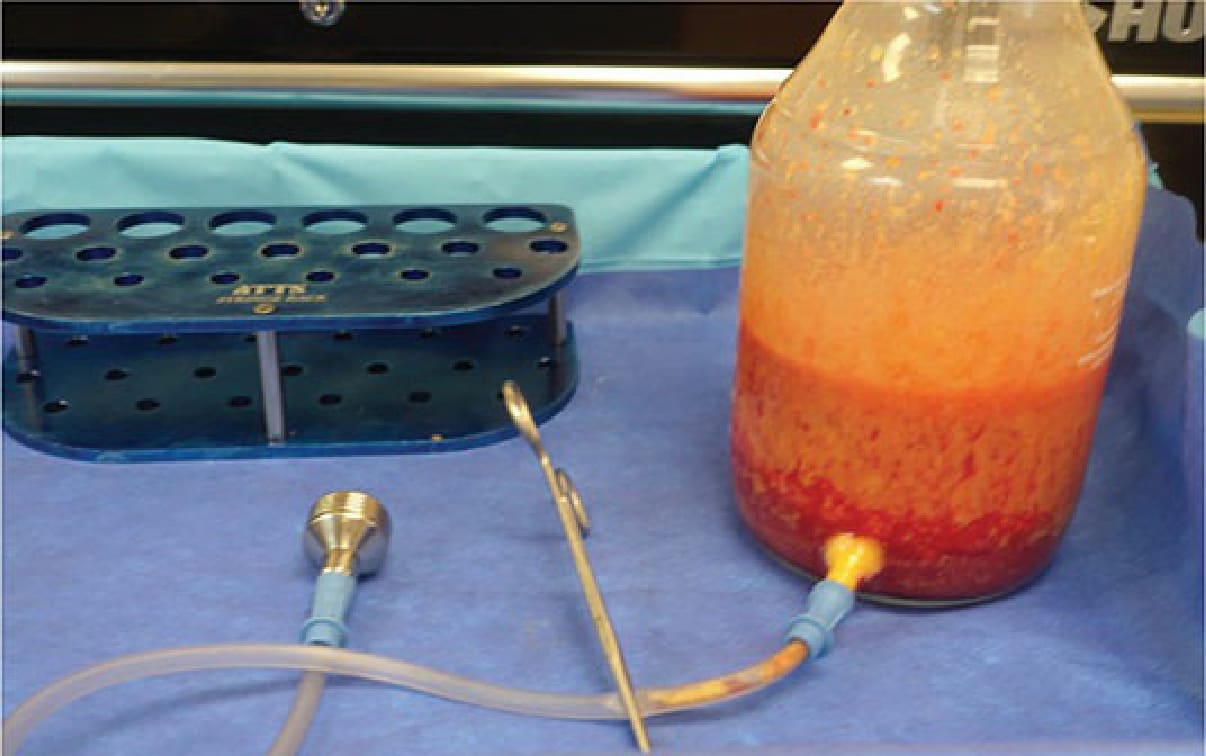
Figure 61-9. First gravity separation—After collection the serous fluid separates by gravity from the fat in the lipoaspirate to the bottom of the harvesting bottle. The lower outlet tubing is unclamped to remove the serous fluid, then reclamped.

Figure 61-10. Preparation of machine-harvested fat for body areas. Harvested fat is transferred to 60-mL Toomey syringes. Harvested fat can also be transferred directly to Luer lock syringes of various sizes.
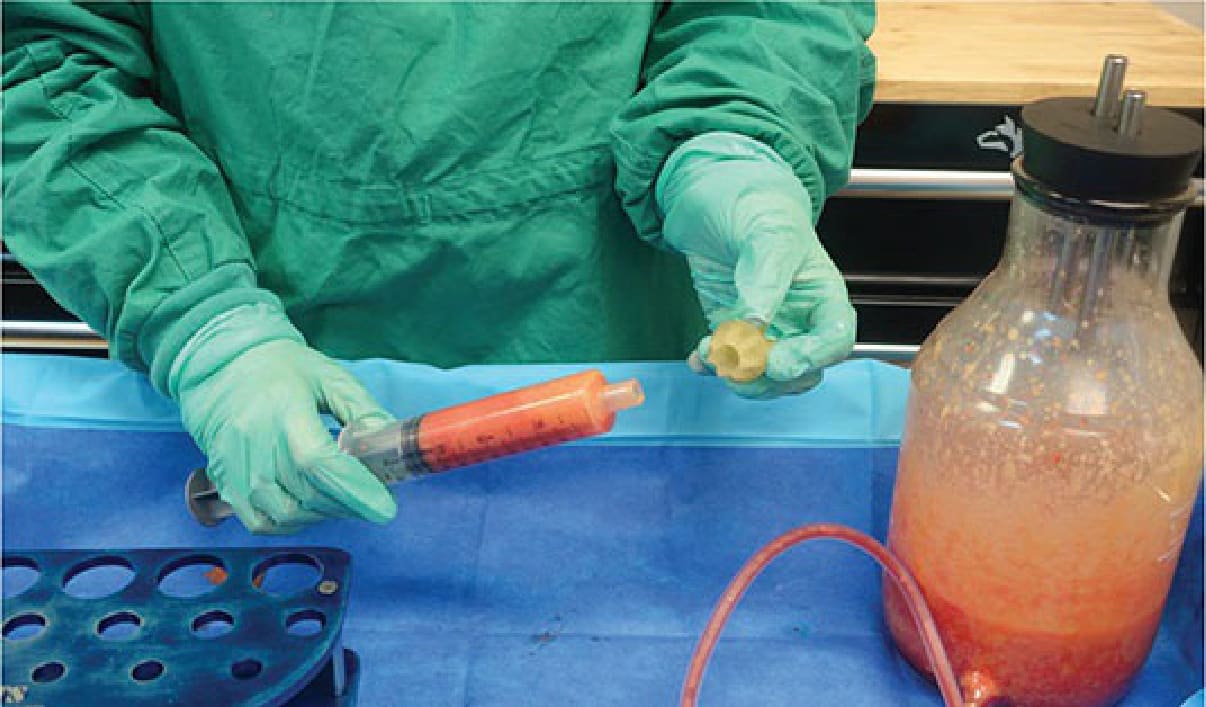
Figure 61-11. Preparation of machine-harvested fat for grafting to body areas—A Toomey syringe cap is placed at the end of the Toomey syringe prior to placing it vertically in the syringe stand to permit additional gravity separation to take place.

Figure 61-12. The Toomey syringe cap is secured in place.
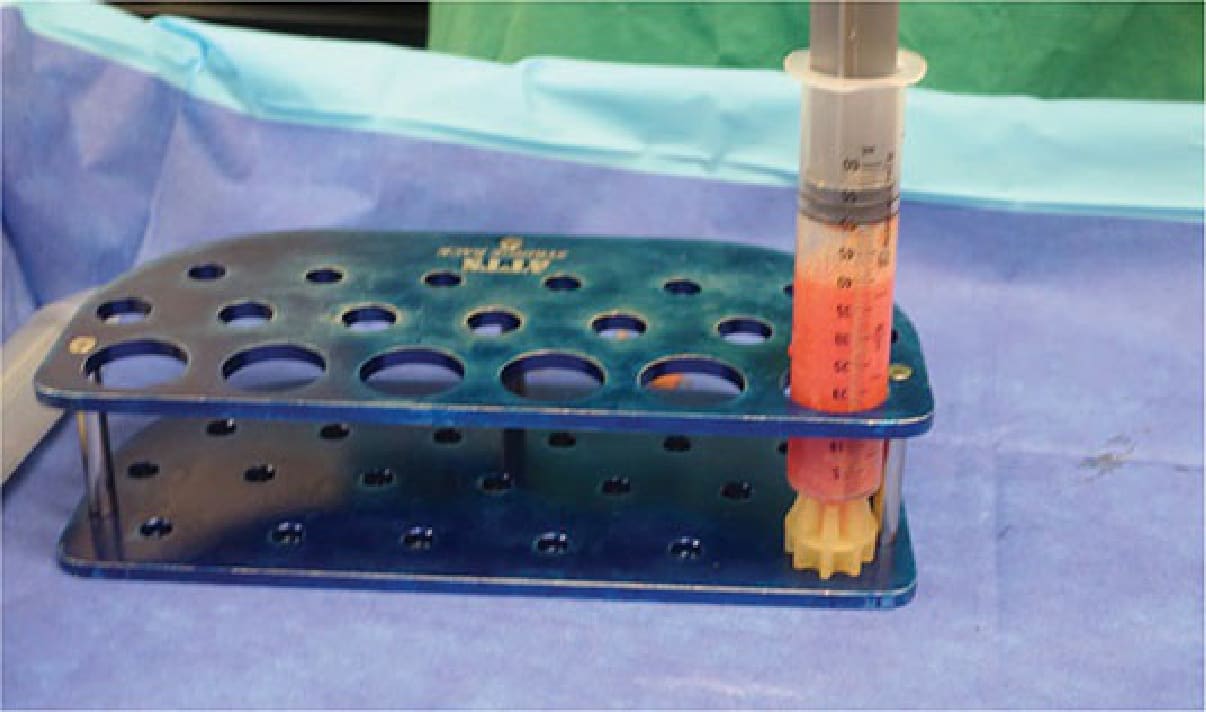
Figure 61-13. The Toomey syringe is placed vertically in the syringe stand to permit gravity separation to take place.

Figure 61-14. Preparation of machine-harvested fat for transfer to body areas: first gravity separation—After collection the serous fluid separates from the fat in the lipoaspirate to the bottom of the harvesting bottle. The tubing attached to the lower outlet can be unclamped to remove the serous fluid, then reclamped.

Figure 61-15. Preparation of machine-harvested fat for transfer to body areas: straining. The lower outlet tubing can be unclamped and the fat can be strained prior to placement into the fat grafting syringes.
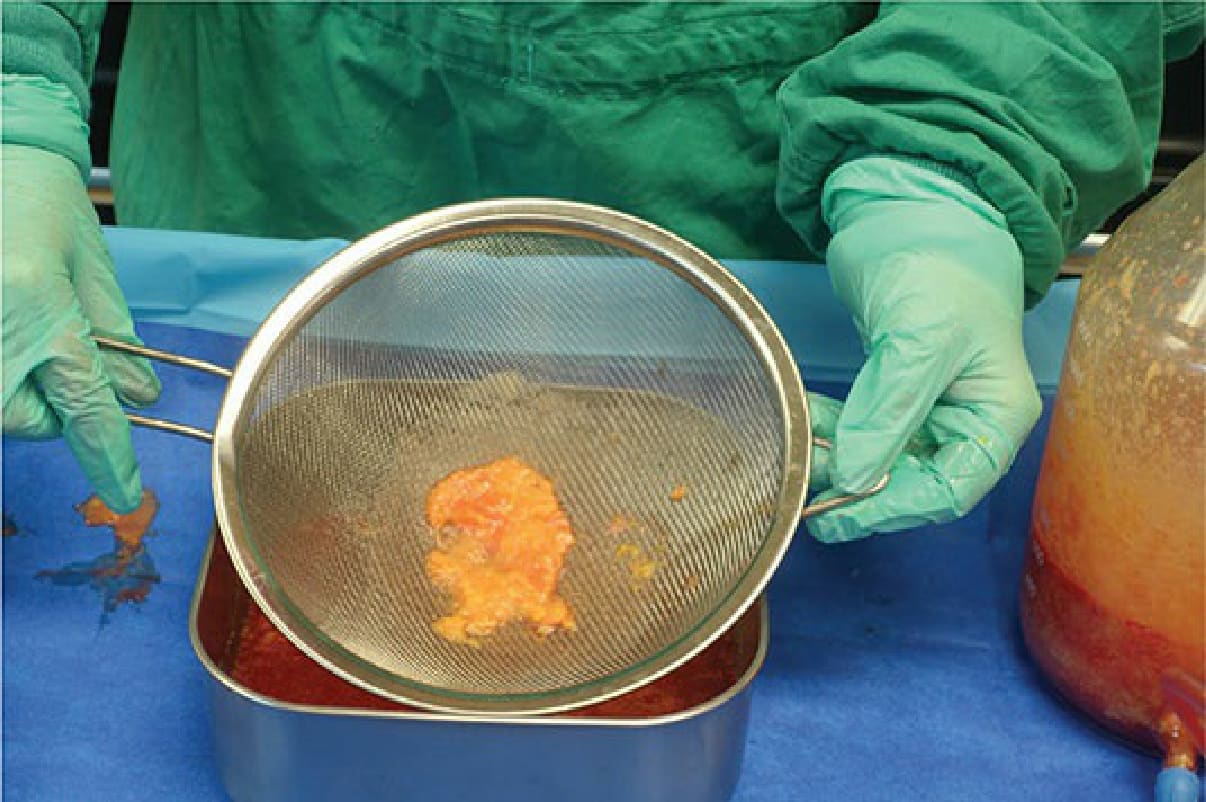
Figure 61-16. Straining harvesting fat—Machine-harvested fat tubing can also be strained to rapidly prepare a large amount of fat for fat grafting to large body areas.
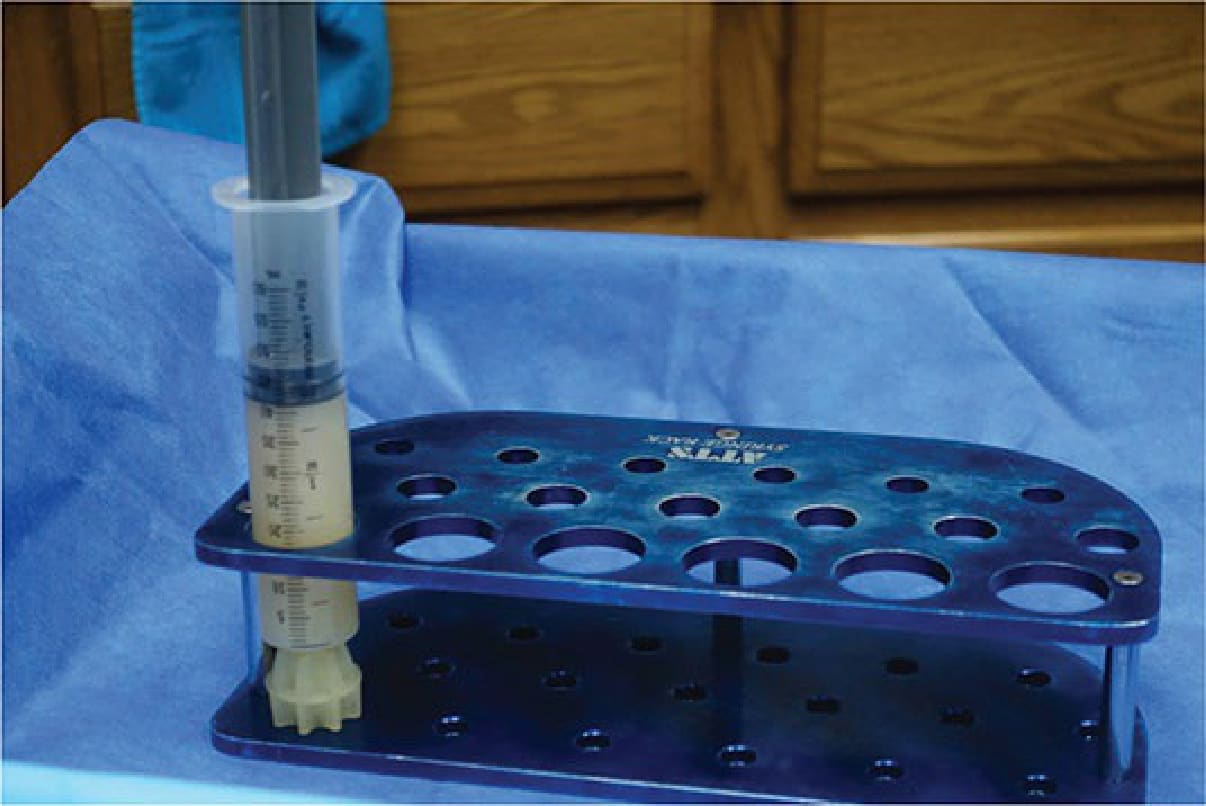
Figure 61-17. Gravity fat harvesting by vacuum pump—A cap is placed at the end of the syringes prior to placing each syringe vertically in the syringe stand. After a Toomey cap is placed on the Toomey syringe, the filled syringe is placed vertically in the syringe stand to permit an additional gravity separation to take place prior to injection.