MALE PHYSIQUE
MALE PHYSIQUE
In contrast to a smooth, soft, and curved female body, a male body is more rectangular/square, tight, and defined. In almost all cultures, a V-shaped male body (more broad and wide upper body as compared to lower abdominals) with defined muscles and minimal fat is desired and found to be uniformly attractive. The male body is defined by the muscles’ shape, which gives it more of an edged/ridged and formed appearance. The HDBC procedure is successful upon complete fat removal in the deep adipose layer (“debulking”) followed by very meticulous removal in the superficial layers over the tendinous insertions of the muscles beneath (Fig. 60-15).
months) with permanent long-term etching of the musculature.
Decreasing fat in an even linear fashion is extremely important so that retraction of the skin is symmetric over the underlying muscle and displays a true etched appearance. Inexperienced surgeons are often nervous to fully reduce this layer and end up only partially doing so, leaving an irregular appearance and one that shows an initial improved appearance but is not maintained long term. For a permanent body change with defined lines, fascial adhesions must be created by aggressive superficial fat removal. The best aesthetic outcome is with a complete understanding of anatomy so that the surgical markings of the fat layers, underlying musculature, and adhesion zones (proposed defined lines) are defined and addressed through the surgery.
Abdominal etching includes aggressive removal of the deep fat layers of the torso, superficial etching of the linea alba (the vertical crease above the umbilicus), the linea semilunaris (the lateral or outside edge of the rectus muscle), the horizontal lines across the tendinous insertions of the rectus abdominis muscle (for the “six-pack”), and hip sculpting (anterior superior iliac spine). Slight irregularities need to be integrated in a defined pattern to ensure a natural look of the abdomen after the etching. It is imperative not to forget liposuction of the mons pubis. The neck/face can also be addressed similarly to a female as preventative treatment.
Chest and chest wall, upper back, sacral, and arm/shoulder areas need to be addressed with any larger fat removal and reshaping to complete the body transformation. Most surgeons will forgo these areas due to the increased surgical and recovery times as well as inexperience in creating definition of these areas.
In men, it is helpful to create a more athletic shape by using harvested fat for muscular definition of the chest and shoulders (to give a more broad upper body appearance and lift the chest), buttock shaping, and calf contouring.11 Fat may be harvested with water and ultrasound-assisted technologies into a filtration system (Puregraft) that removes debris such as oil, connective tissue, and blood to obtain the most pure fat for harvesting. PRP is added to the fat in a 2–4:1 ratio to possibly help survivability and longevity.
Finally, the male breast glands should be removed if they are evident after lipocontouring of the breast and fat injection into the muscle.
Poor planning and anatomical consideration in a prior male abdomen HDBC surgery
To create an abdominal six-pack or “V-taper” in a younger male desiring a more contoured abdomen, it is essential to identify all the tendinous insertions of the rectus muscles and aggressively define these areas while leaving a small amount of fat over
the muscle bellies themselves (Figs. 60-16 and 60-17). Improper placement of presurgical markings can lead to an incomplete abdominal six-pack shape, and uneven resection of the superficial adipose layer can lead to fibrotic bands in the wrong location causing superficial irregularities often seen best during flexion/extension (Fig. 60-18A and B).
Planning and anatomical considerations in a male chest revision surgery
The male chest requires four steps to obtain the best contouring: (1) VASER ultrasound, (2) Rotary power-assisted liposculpting, (3) Fat injections with PRP to the chest musculature, (4) male breast gland removal (Fig. 60-19). In this instance a patient had a traditional approach of minimal hand aspiration liposuction to the chest with overresection of the male breast glands leading to a “flat” appearance without contour. To repair this, HDBC of the chest and chest wall was performed in the superficial layer to define a new lower and lateral border of the chest. Fat was harvested and injected into the upper pole of the chest for lift and volumization as well as behind the nipple to give projection. Additionally, fat was injected into the shoulders to give the upper body a more broad appearance.

Figure 60-15. Athletic male high definition body contouring with tight skin. Men with an athletic body shape and muscular definition before (left) a high definition procedure get contouring results quickly (right, here seen at 3

Figure 60-16. Men with a slightly higher baseline body fat percentage also benefit significantly from etching and high definition body contouring.

Figure 60-17. Athletic male six-pack and “V-taper.” Six months result showing high definition athletic shape of the abdominal musculature with tapering at the lower abdominals and hips. Proper placement of markings over anatomical landmarks with both deep suction and superficial etching gave an optimal outcome.
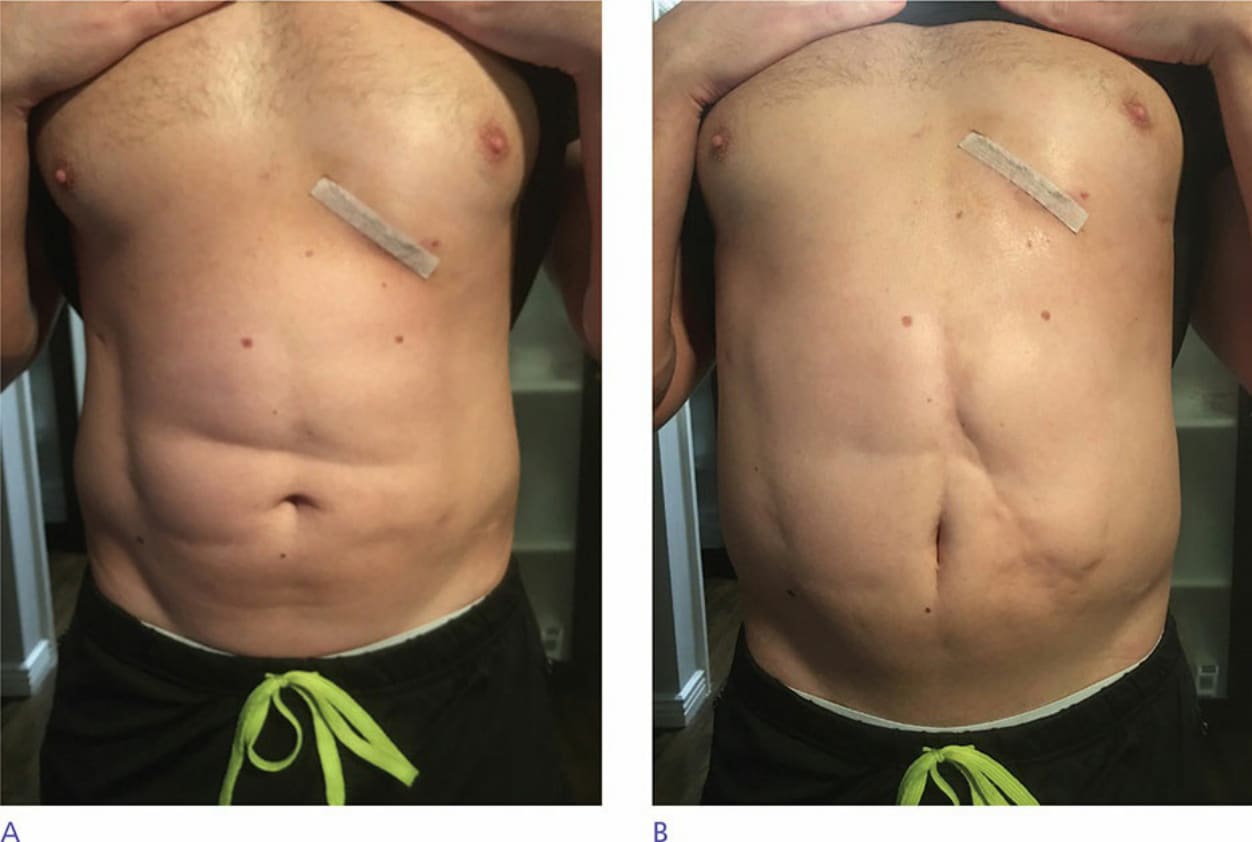
Figure 60-18. (A and B) Athletic male six-pack with poor outcome. Six months result showing abdominal musculature without proper etched lines and fibrosis and asymmetry worse with extension. This outcome was due to inappropriate liposuction of the superficial fat and poor removal of the deep layers without contouring. This is an example of a poor cosmetic outcome from another cosmetic surgeon that will require revision surgery to repair.
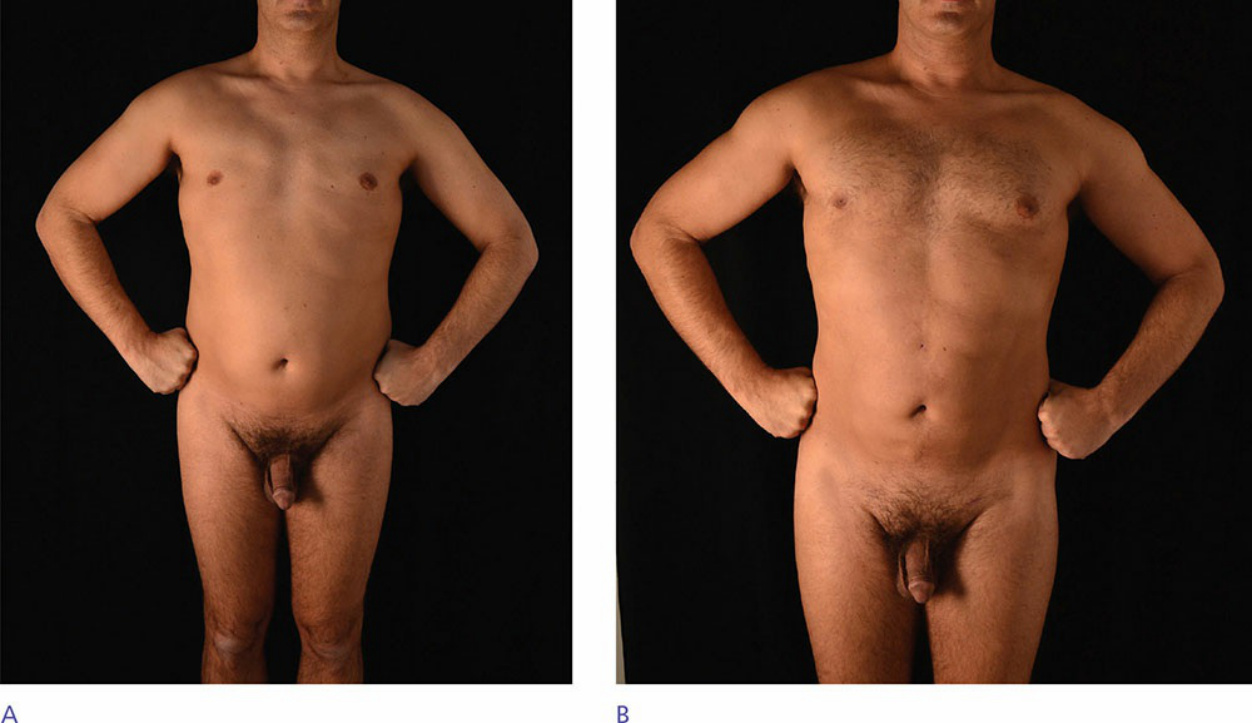
Figure 60-19. Male chest high definition body contouring revision. Fat harvesting of the chest and shoulders with sculpting liposuction of the lower chest, chest wall, and shoulders to give improvement in upper body shape and muscular definition. (A) Pre-procedure. (B) Post-procedure.