Silicone
Silicone
Injection of silicone (polydimethylsiloxane, PDMS) has a storied past, and its use as a soft-tissue implant continues to be controversial. The term silicone refers to a family of inert, silicon-containing synthetics. Siloxanes are members of this family, composed of silicon, oxygen, and methane. For any given compound, the siloxane chain length and polymerization determines its viscosity, measured in centistokes (cs). The viscosity of water equals 1 cs and 350 cs for mineral oil. Heavy metals, oils, and other organic substances naturally contaminate silicones, so purification is compulsory. Proponents of silicone injection for augmentation believe that many of the reported adverse reactions result from impurities and that it is safe and effective in the hands of experienced providers who administer small quantities of product.
Permanent augmentation with PDMS became popular in the 1960s with the introduction of medical grade products. Soon, untrained practitioners began injecting industrial silicones or adulterated oils instead, which caused severe complications. Medical grade liquid injectable silicone has a viscosity of 350 cs and is purer than industrial compounds. Despite clinical trials, it was never FDA-approved for use in humans. AdatoSil® (5000 cs) and Silikon® (1000 cs) were approved in 1994 and 1997, respectively, for ophthalmologic indications and have been injected lawfully for soft-
tissue augmentation since 1997, when the FDA passed the Modernization Act allowing off-label use of medical devices. Silikon 1000 is currently the most appropriate agent available.
The technique is paramount when administering permanent fillers. The microdroplet serial puncture method allows for more precise placement: 0.005 to 0.01 mL aliquots deposited every 2 to 5 mm subdermally (Fig. 58-9). Overcorrection or multiple passes should be avoided. Relatively small volumes are recommended, and in a given treatment session, no more than 0.5 mL should be used for regions with small surface area defects (i.e., the nasolabial folds), and up to 2.0 mL may be used for regions with large surface area defects (i.e., facial lipoatrophy). These volumes decrease over time as the desired effect is achieved. Treatment sessions typically occur every four weeks initially and then can be spaced farther apart to allow sufficient time for fibroplasia to encapsulate the product.54
Risks related to silicone augmentation are real but often secondary to improper technique, incorrect dosage, or tainted material. Erythema, edema, and ecchymoses are common and usually resolve within days. Dermal, instead of subdermal, injection can cause rippling. Other potential complications include superficial beading from overcorrection, granuloma formation (Fig. 58-10), and product migration, which is more likely with large amounts of less viscous oil. Meticulous treatment protocols
frequently help avoid these adverse events,55 yet delayed granulomatous reactions weeks, months, or years after treatment are possible and may require intralesional corticosteroids combined with 5-fluorouracil, and possibly systemic antibiotics.
Amid decades of debate, recent studies suggest that when injected under optimal conditions, the complication rate from silicone soft-tissue augmentation is less than 1%. In expert hands, highly purified injectable silicone is a reliable and reproducible option for correction of advanced HIV-associated lipoatrophy.27,56
COMPLICATIONS
Given that facial rejuvenation is largely an elective procedure, the safety of soft-tissue fillers is paramount. Significant adverse events are infrequent. Possible complications and methods of addressing them are listed in Table 58-6.
Pain, erythema, edema, induration, bleeding, and bruising are the most common reactions. They are generally mild and resolve within 1 week. Intense physical activity that raises blood pressure may increase the incidence of ecchymoses and bleeding, so patients should abstain for 24 hours postprocedure. Limiting the number of needle sticks, using blunt-tipped cannulas or small gauge needles, slowly injecting small volumes of product, and temporarily holding unnecessary antiplatelet medications/supplements for the 7 to 10 days prior to treatment may help minimize these risks.57 When bruising does develop, energy based therapies (i.e., pulsed-dye or
potassium titanyl phosphate lasers, intense pulsed light) may clear extravasated blood more rapidly.58
In addition to injection site reactions, more serious complications occur at low rates. Intradermal placement can produce ridging, beading, and palpable or visible papulonodules. Superficial HA in particular can cause a temporary bluish tint in these areas due to the Tyndall effect—differential refraction of light off particles in a colloid (Fig. 58-11). Persistent papulonodules are more likely with Sculptra, Bellafill/Artefill, and silicone than other agents.
Infections, including cellulitis and abscesses, are another potential risk. Puncture sites can serve as portals of entry for resident skin or oral flora. Sterilizing the treatment area with isopropyl alcohol, chlorhexidine or another appropriate antiseptic and wearing clean gloves are common practice to minimize infection rates. All suspected infections should be cultured and/or biopsied for identification and sensitivities. Patients should start broad-spectrum antibiotics with or without anaerobic coverage until the results return.59 Incision and drainage may be needed for fluctuant lesions. Injection-related trauma can also reactivate herpes simplex virus, particularly periorally. In those with a history of frequent or post-procedural outbreak(s), prophylactic antiviral therapy may be warranted, and injection should be delayed in the case of active blistering.58
In the early era of soft-tissue augmentation, hypersensitivity reactions were far more frequent. Bovine collagen was the first FDA-approved soft-tissue filler in the United States, but 3% of patients developed antibodies and clinically significant allergy to the material.60 Thus, skin testing was mandatory to decrease, albeit not fully prevent, this risk. In the United States, Bellafill/Artefill is the only currently marketed product still requiring skin testing before augmentation. Part of the appeal of HA, Sculptra, and Radiesse is their biocompatibility, a quality that eliminates the need for preprocedural allergy testing. A few cases of hypersensitivity to HA do exist and may arise from contaminants, by-products of bacterial fermentation used in production, or lower– molecular-weight molecules such as those in Juvederm Voluma XC.59,61 While these reactions may subside spontaneously, topical calcineurin inhibitors, intralesional
corticosteroid injections, systemic anti-inflammatory medications, incision and drainage, or hyaluronidase injection can hasten the process.57
Both hypersensitivity and infection with or without biofilm can contribute to the formation of delayed nodules. Foreign-body reactions are another possible explanation, and distinguishing between these etiologies can be difficult. Unlike acute abscesses, biofilms lead to chronic infection. Microbial colonies adhere to the implant and secrete an extracellular polysaccharide matrix coating that is resistant to detergents, antimicrobials, and host immune responses. Clinically, nodules related to biofilms may appear inflammatory, infectious, abscess-like, or granulomatous.59 Because conventional culturing methods frequently fail to detect the underlying bacteria, culture results may be misleading. Fluorescent in situ hybridization (FISH) detects the causative microbe in most culture-negative cases, but is not routinely run.62 Atypical mycobacteria can cause delayed infection as well, so separate histology and tissue cultures should be considered. Results from these studies should guide the ongoing treatment.
Any time a foreign body is introduced into the skin, there is potential for a nonallergic granulomatous reaction, even years after treatment. The incidence after HA correction has been reported as 0.02% to 0.4%.63,64 It is higher for non-HA materials.63 As previously mentioned, volume injected, presence of impurities, and product type affects the rates of granuloma formation. HA and collagen typically develop cystic granulomas; silicone, paraffin, and polyacrylamide (not licensed in the United States) lipogranulomas; and PMMA and poly-L-lactic acid sclerosing granulomas.63 Since differentiating inflammatory complications from biofilm infections is not straightforward, antibiotic treatment, such as clarithromycin or a tetracycline class medication for 2 to 6 weeks, rather than corticosteroids should be first line, and longterm antimicrobials may be prudent in suspect infections.65
Fortunately, most contour irregularities, blue-gray discoloration, and acute and delayed nodules improve over time either spontaneously or with treatment. One of the appealing features of HA derivatives is the ability to reverse undesired outcomes with hyaluronidase (Fig. 58-12). There are two FDA-approved formulations, Vitrase and Hylenex, used off-label as first-line treatment to degrade injectable HA. Vitrase is a purified ovine testicular enzyme, while Hylenex is a recombinant human protein. The necessary hyaluronidase dose varies by formulation and filler. In vitro data suggest that more cross-linked HA derivatives require larger doses for optimal outcomes. It is reasonable to use 5 units of Vitrase hyaluronidase per 0.1-mL Restylane and 10 units per 0.1 mL of Juvederm.26 Allergic reactions to hyaluronidase are rare, estimated at 1 in 2,000,65 and the majority of these are localized. In nonemergent situations, intradermal skin testing may be considered, especially in patients with known allergies to bees, wasps, or hornets (classification order Hymenoptera), whose venom contains
hyaluronidase. Those allergic to thiomersal are also at increased risk, since some enzyme formulations contain this preservative.65 If intralesional hyaluronidase is ineffective or nodules occur in the setting of non-HA augmentation, other reported medical therapies include oral antibiotics (antimicrobial and anti-inflammatory effects); topical, intralesional, or systemic corticosteroids; intralesional 5-fluorouracil; oral immunosuppressants such as cyclosporine; lasers; or combination therapies.66 Persistent or refractory nodules may require excision.
Though rare, potentially irreversible vascular complications are the most dreaded and serious adverse events following soft-tissue augmentation.67 Vascular compromise from extravascular compression, intravascular injection, or embolism with downstream occlusion can cause tissue ischemia and necrosis. The glabella is a high-risk, watershed region due to limited collateral circulation.68 Historically, up to 50% of patients treated with Zyplast to the glabella developed some degree of necrosis.69 Injection at the medial cheek similarly demands care.68 The angular artery, a terminal branch of the external carotid, runs superior to the nasolabial fold then divides into the lateral nasal artery as well as other collateral branches that anastomose with the internal carotid system. Substantial anatomic variation in the exact course of these vessels exists. Moreover, the union of embryonic fusion planes at the alar groove prevents tissue distension, so there is little room to accommodate large quantities of filler without interrupting the vasculature.67 Acute or excruciating pain, blanching, duskiness, and reticulate erythema (Fig. 58-13) tracking the involved artery and its tributaries may indicate impending necrosis. Typically, these signs occur immediately but can be delayed in the case of occlusion from postprocedural edema. Once recognized, treatment should begin immediately.57 Prompt and ongoing care decreases the risk of permanent adverse effects and disfigurement.67 One study recently reviewed several cases of vascular compromise and outlined treatment and prevention measures.67 Because of its ability to decrease edema and consequently, external vessel compression, some recommend hyaluronidase injection irrespective of filler type.70 Early reports supported infusion of up to 30 U of enzyme along the affected vasculature,71 but now the recommendation is to exceed 100 to 200 units.70,72,73 The more cross-linked the HA agent, the more hyaluronidase necessary for optimal outcomes.26 Application of warm
compresses and topical nitroglycerin, as well as firm massage, are other recommended treatments. Oral aspirin, prednisone, and hyperbaric oxygen, and low–molecular-weight heparins have been employed less frequently. Meticulous wound care is important if necrosis and ulceration do develop.
Alternatively, filler implanted intravascularly can embolize retrograde into the ocular circulation, a rare cause of ophthalmoplegia or blindness.74 Incidence of this complication was reported as 0.001% in the past, but the largest recent review of cases performed by expert physicians found a rate of 0.05%. This increased rate may be partially attributable to the introduction of newer agents designed for deeper deposition.67 Correction at the glabella, nasal dorsum, or nasolabial folds are at highest risk,75 since branches of the internal carotid (i.e., supratrochlear and dorsal nasal arteries) either directly feed or anastomose at these anatomic locations. The internal carotid also gives rise to the ophthalmic artery and the central retinal artery; hence, injecting under high pressure can force product upstream into the ocular circulation74 and produce sudden, profound pain and vision loss. More infrequently, forceful intraarterial administration can cause cerebral artery embolism with potential infarct. Patients should undergo emergent ophthalmology and/or neurology evaluation if there is any concern for impairment; immediate retro- or peribulbar injection of at least 500
units hyaluronidase is one technique proposed to reverse partial vision changes.76
Preventing vascular compromise is critical, considering that treatment of local tissue necrosis, blindness, or cerebrovascular infarct is often ineffective once it has occurred.74 Using blunt-tipped cannulas instead of needles is one way to decrease potential risks. The cannula’s flexible, dull end is less likely to pierce vessel walls and place fillers intralumenally. Cannulas may be especially prudent for subdermal injection at the central cheek medial to the mid-pupillary line.
Overall, facial rejuvenation with injectable fillers and implants is a safe procedure. Understanding regional anatomy, injection techniques, and methods to prevent and manage complications ensures successful outcomes.

Figure 58-9. Silicone correction in a patient with human immunodeficiency virus (HIV).

Figure 58-10. Nodule formation after silicone injection.

Figure 58-11. Tyndall effect at the tear troughs from superficial deposition of hyaluronic acid filler. Baseline (A) and after (B) hyaluronidase injection.

Figure 58-12. Correction of contour irregularities with hyaluronidase. Baseline (A) and after (B).

Figure 58-13. Evolving vascular compromise with dusky, reticulate erythema.
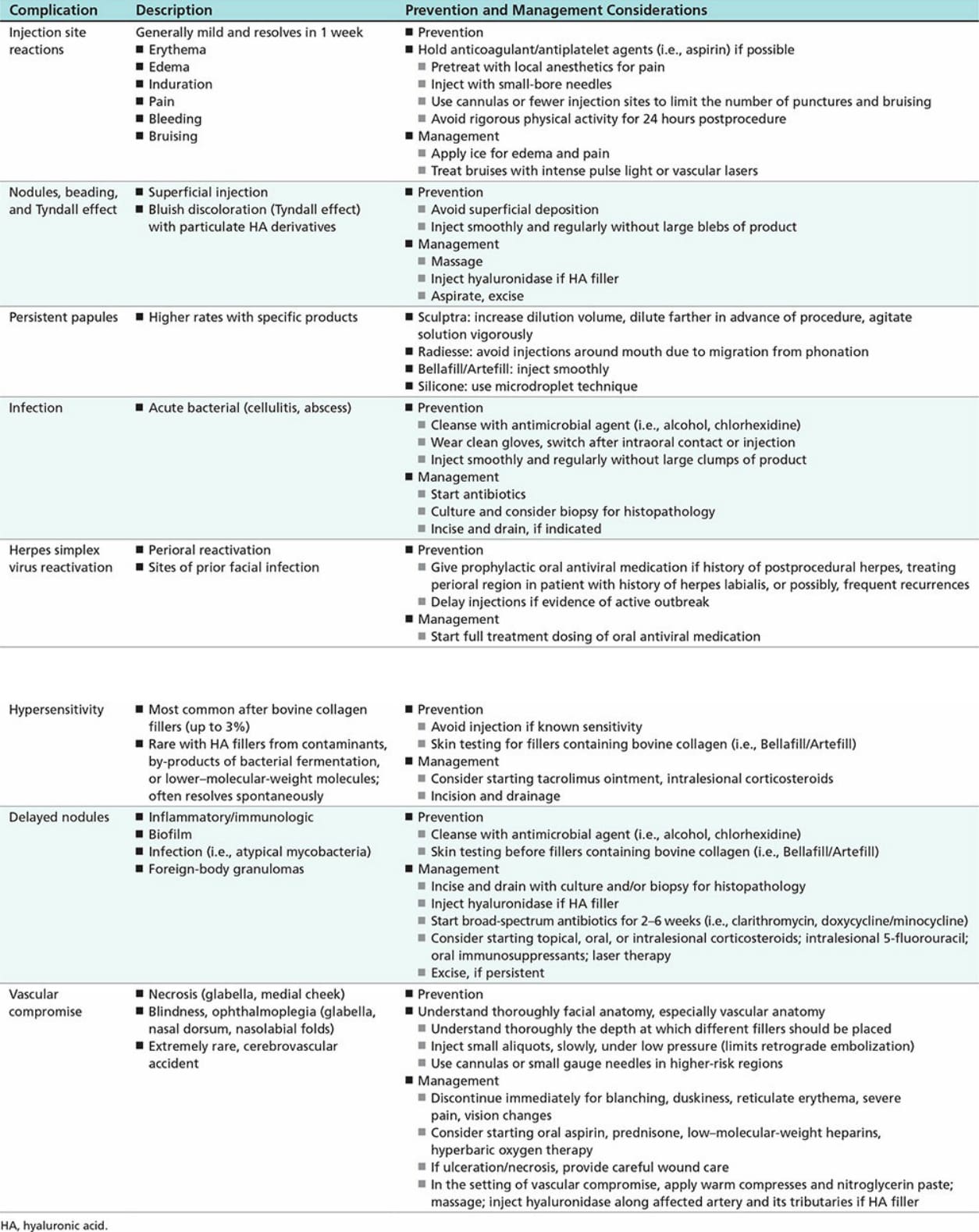
Table 58-6. Complications from Soft-Tissue Fillers