Pertinent vascular anatomy
Pertinent vascular anatomy
In addition to knowledge of multiple injection techniques, expert practitioners should have a detailed grasp of relevant vascular anatomy in an attempt to avoid devastating adverse events. This has been investigated in detail in the past,8 and some of the most high-risk and frequently discussed regions are addressed in Figure 58-1.
The majority of facial blood supply comes from branches of the external carotid artery, which anastomose with divisions off the internal carotid artery at the nose. The facial artery is the most studied and frequently compromised branch of the external carotid. It extends along the mandible up toward the medial canthus under the platysma, zygomaticus major, and lip elevator muscles to terminate in the angular artery that runs along the lateral nose. These landmarks are general guidelines, however, and the path is tortuous with substantial individual variation,9,10 so care must be taken when injecting at
the medial cheek and along the nasal sidewall because there is a higher risk of arterial occlusion. Blunt-tip cannulas that do not pierce vessel walls as easily as needles may be safer in these regions, though this has yet to be definitively established.
The angular artery supplies the nasal sidewall before joining with the dorsal nasal artery, one of two divisions of the ophthalmic artery, at the root of the nose. The latter continues down the nose, irrigating its root and dorsum, before anastomosing with the lateral nasal artery, a branch of the facial artery. There have been reports of retrograde emboli and blindness due to these interconnection and again, care must be taken to inject small aliquots under low pressure periosteally and perichondrally along the nose.
Similarly, anastomoses between the cutaneous and ophthalmic circulation in the upper face may lead to blindness and even cerebrovascular deficits. Both the supraorbital and supratrochlear arteries branch off the internal carotid near the glabella. The supraorbital emerges from the supraorbital notch just medial to the mid-pupillary line, while the supratrochlear lies beneath the medial most glabellar rhytid. They run along the bone for approximately 1 cm, then pierce the frontalis muscle and branch superficially. Hence, injections at the medial portion of the upper face should only be performed with cannula or superficially in the dermis, while those in the mid-to-upper portion of the forehead should be periosteal deep to the level of the vasculature. As with the dorsal nose, complications occur from direct injection into or compression of the vessels or retrograde emboli into the ophthalmic and then terminal retinal arteries off the internal carotid.
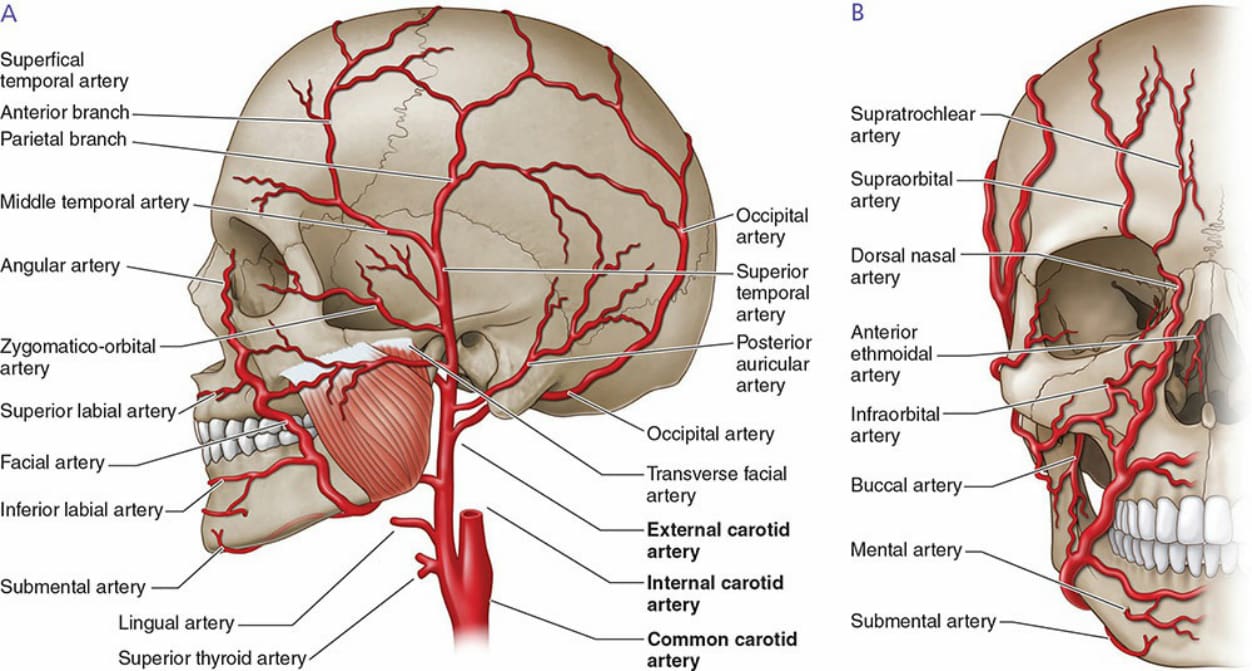
Figure 58-1. Anstomoses of the internal and external carotid circulations.