Preoperative assessment
Preoperative assessment
Prior to initiating BTX treatment, the patient must be thoroughly assessed for contraindications and educated in terms of goals and expectations. Contraindications to BTX include:
- Known hypersensitivity to BTX or any of the components in the formulation
- Active infection at the injection site
- Neuromuscular diseases such as myasthenia gravis, Eaton–Lambert syndrome, or
amyotrophic lateral sclerosis, which may increase risk of generalized muscle weakness, diplopia, ptosis, dysphonia, dysarthria, severe dysphagia, and respiratory symptoms
4. Pregnancy and lactation (pregnancy category C)
Patient education remains one of the most crucial steps to the success of any dermatologic surgical procedure. First-time BTX patients may arrive with a variety of preconceptions, and it is the responsibility of the dermatologic surgeon to provide safe and appropriate guidance toward achieving individual goals. Important areas to consider include: establishment of realistic goals, assessment of desired treatment area, understanding of expectations and potential side effects, written informed consent, and photographic documentation.
First, priority should be given to developing trust and rapport with the patient, and a thorough understanding of their treatment goals. At this stage, it is important to identify those patients who may have an element of body dysmorphism, as this syndrome has a small but significant prevalence in dermatology offices.40 Treatment of patients with unrealistic goals should be avoided.
Next, a careful evaluation of the treatment area should be conducted with the patient being an active participant in the examination. One effective technique is to have the patient look into a handheld mirror while explaining the difference and interrelation between dynamic and static rhytides. It is important for the patient to understand that improvements in dynamic rhytides will likely be swift and sure, but static lines will often require multiple treatments over a more prolonged time course. By actively engaging the patient in this assessment and conversation, the dermatologic surgeon can also highlight the long-term benefits of BTX therapy in the treatment of facial rhytides.41 In almost all cases of BTX treatment, clinical effects will be temporary, and repeated
treatment sessions will be required to maintain or achieve a certain aesthetic goal. This remains an important concept to explain during patient education. Simple side effects such as bruising and swelling should always be mentioned whereas discussion of other complications should be guided in a focused manner in keeping with the patient’s baseline clinical status and the specific type of BTX treatment being administered. The dermatologic surgeon should always leave ample time for answering patient questions and concerns.
Once the patient has been thoroughly educated and a treatment plan agreed upon, written informed consent should always be obtained. Photographic documentation is highly recommended for both pre- and posttreatment status and can be obtained either by standard digital photography or dedicated imaging devices. In the case of facial rhytid treatment, it is often useful to schedule a 2-week follow-up appointment at which time minor touch ups (if required) can be administered. This can also help to avoid unnecessary patient anxiety during the immediate postoperative period when the treatment begins taking effect. After treatment, patients should be counseled to avoid lying down, manipulating the area, or undergoing strenuous physical activity for a period of 4 hours. In-office ice packs can be offered to decrease swelling.
Treatment
The most popular dermatologic uses of BTX include the reduction of facial rhytides, facial contouring, and treatment of focal hyperhidrosis. However, BTX can also have pleasing effects on the neck and chest, scars and wounds, pre-existing or iatrogenic facial palsies and asymmetries, body contouring, and skin boosting.
Injection technique The patient is seated upright or slightly tilted for comfort in an examination chair with an elevated head rest. Prior to injection, the skin should be cleansed with an antiseptic agent such as 70% alcohol or 4% chlorhexidine gluconate. The treatment area should be identified and muscular patterns may be marked with a skin marker. Each patient potentially presents with subtle anatomical differences, and these should guide the dermatologic surgeon in delivering optimally tailored treatment regimens. Variations in muscular patterns in the upper face are well established,42,43 and studies have demonstrated that targeted individualized treatment delivers superior outcomes.44 Some injectors advocate the use of real-time imaging aids to identify and avoid vasculature while injecting so as to minimize the possibility of bruising, though there is no evidence to suggest an impact on outcomes.45 Additionally, ultrasound examination may be helpful to guide injections directly into muscle bellies.46 For the majority of patients, these adjunctive techniques are unnecessary for successful treatment.
Several techniques may be used to decrease injection pain, including application of ice pack just prior to injection, cold air prior to and during injection, mechanical distraction, or topical anesthesia. Simple mechanical distraction administered by an assistant tapping on the patient’s shoulder or forehead during injections is a highly effective and efficient way to decrease injection pain. In general, BTX should be delivered intramuscularly, although due to diffusion, perimuscular or subcutaneous placement of medication may sometimes be acceptable.47,48 For most facial applications, the optimal needle for injection is a 32-gauge 0.3-mL insulin syringe (Becton, Dickinson and Company, Franklin Lanes, NJ), though other needles may be used as well.
Due to the interrelationship between the facial musculature, it is useful to conceptualize the upper and lower face as global treatment regions rather than focus on a specific area such as the glabella or lateral canthus. This mindset promotes the goal of achieving a harmonious, balanced, natural and aesthetically pleasing outcome.
Upper face Treatment of the upper face includes the glabella, the lateral canthus, the forehead, the infraorbit, and the bunny lines.
Glabellar frown lines The glabellar frown lines form secondary to hyperactivity of the procerus, corrugator supercilii, and depressor supercilii muscles. Treatment in this area can relax these wrinkles and relieve a habitually angry or displeased expression. Three to five injection points should be used depending on the patient’s presenting muscular pattern (Fig. 57- 1). One study demonstrated no additional benefit to five injection points over three.49 In order to limit complications such as ptosis, injections should be placed medial to the mid-pupillary line and 1 cm above the eyebrow. A typical starting dose for the majority of patients is 20 units of ONA,50 50 units of ABO,51 or 20 units of INCO.52 Use of lesser amounts of medication has been correlated with reduced effect duration and patient satisfaction.53–56 However, the most important guiding principle for treatment dosage remains the clinical assessment of what is required to achieve a certain aesthetic goal (Fig. 57-2).
There are several considerations when treating glabellar frown lines. Men tend to require higher dosages due to increased muscular activity.57 Race does not have an impact on treatment efficacy.58–60 Isolated treatment of glabellar frown lines can lead to dramatic, and sometimes unwanted, changes in eyebrow position61 which can be balanced with treatment of the forehead and/or lateral canthus. The long-term benefits of repeated glabellar frown line treatments at regular intervals include reduction of static rhytides and improvement in skin texture and quality.62–64
Lateral canthal lines Excessive lateral canthal lines (sometimes referred to as “crow’s feet”) can give the impression of an aged and tired appearance. They are secondary to hyperactivity of the orbicularis oculi muscle and typically present as a fan-shaped pattern radiating from the lateral canthal region.42 Treatment with BTX in this area should be delivered in one to five injection points that are placed superficially 1 to 1.5 cm lateral to the orbital rim (Fig. 57-3). Once again, treatment dosage should be determined clinically, but a typical starting point to each side is 12 units of ONA,65,66 36 units of ABO,67,68 or 12 units of
INCO.69,70 Much lower dosages may be effective as well. In this area, minimizing injection points can help to reduce pain and side effects while maintaining equivalent efficacy.68 As with glabellar frown lines, repeated and regular BTX treatment in the lateral canthal region confers long-term benefits.64 One important consideration in this area is that many patients present with significant inferolateral extension of lateral canthal lines down toward and across the zygoma. These rhytides should not be “chased” with BTX due to risk of denervation of the zygomaticus muscle and resultant facial asymmetry (Fig. 57-4).
Horizontal forehead lines Horizontal creasing along the forehead is a cause of concern for many patients presenting to dermatology clinics. This phenomenon is caused by hyperactivity of the frontalis muscle. Treatment with BTX in this area is typically delivered over four to eight injection points with small doses ranging from 2 to 8 units of ONA, 5 to 20 units of ABO, or 2 to 8 units of INCO (Fig. 57-5).71 The goal of treatment is to soften existing wrinkles while avoiding freezing of all expressiveness or induction of brow ptosis. The
most feared complication of isolated frontalis treatment is brow ptosis. In order to avoid this complication, careful assessment of the patient is required. Some patients will present with smaller foreheads, naturally low brows, minimal frontalis bulk, or exhibit the tendency to overutilize the frontalis muscle for brow elevation when making facial expressions. These features must be noted prior to treatment and should lead the dermatologic surgeon to consider lowering treatment dosage or placing injection points higher on the forehead approaching the hairline. Another way to minimize risk of brow ptosis is to simultaneously treat the glabellar region in order to balance the muscles of the upper face. In the majority of cases, this is the most reliable way to achieve a beautiful outcome.72 Simultaneous treatment of the glabellar region serves to prevent brow ptosis as well as relax central horizontal forehead lines (Fig. 57-6).
Bunny lines and infraorbit Hyperactivity of the upper nasalis muscle produces a horizontal or fan-shaped pattern of rhytides at the radix of the nose, sometimes referred to as “bunny lines.” This concern can be addressed with 2 to 3 units of ONA (or equivalent ABO or INCO) injected in two injection points in the superior nasalis muscle.73 Caution should be taken to maintain the injection points at least 1 cm above the nasolabial fold to minimize the risk of affecting lip elevators which may result in unwanted lip ptosis.
The immediate infraorbital region can be treated with BTX with the aim of targeting the pretarsal portion of the orbicularis oculi muscle. Hypertrophy of this muscle can be associated with a decrease in the size of the palpebral aperture. Two units of ONA placed 2 to 3 mm inferior to the lower eyelid margin along the mid-pupillary line is typically sufficient to relax infraorbital wrinkling and subtly increase the palpebral aperture (Fig. 57-7).74,75
Lower face Common concerns in the lower face that are amenable to BTX therapy include excessive nasal flare, nasal tip droop, perioral rhytides, upper gum show, hypertrophic masseters, depressed oral commissures, and wrinkled chin.76
Nasal tip droop A plunging nasal tip can be due to an overactive depressor septi muscle and can give the impression of a shortened upper lip especially while smiling. For patients who are not candidates for rhinoplasty, BTX represents a simple alternative to improve this issue. Two to 10 units of ONA should be delivered at the columella-labial angle for this purpose.77,78
Perioral rhytides The orbicularis oris is a circular muscle that extends circumferentially around the oral aperture and is primarily responsible for the development of hyperdynamic vertical perioral rhytides. Treatment of this muscle with judicious amounts of neuromodulator can achieve temporary improvement of these lines. An early uncontrolled open-label trial79 studied 18 patients who had received between 7 and 18 units of onabotulinumtoxinA (ONA) to the perioral region. Effacement of perioral wrinkles and enhanced lip eversion and fullness was observed. More recently, a randomized, doubleblind trial demonstrated that a dose of 7.5 units of ONA distributed in several injection
points periorally was sufficient to achieve the desired clinical effect.80 Often, total dosages ranging between 4 and 6 units of ONA (or equivalent neuromodulator) are used. One unit aliquots are delivered over four injection points along the superior vermilion border and two injection points are used along the lower vermilion border, staying 1 cm medial to the oral commissure to avoid unwanted spread into muscles inserting into the modiolus (Fig. 57-8). Prior to moving forward with treatment, patients are warned that they may have difficulty pursing their lips, pronouncing their “p’s,” drinking out of straws, and playing a wind instrument. A minimal amount of units is used initially since a second treatment, if necessary, can be performed a week after the first injection session and is preferable to overtreating with resultant excessive muscle paralysis in a single treatment session.
Upper gum show Excessive gingival display when smiling is a result of hyperactivity of the levator labii superioris alaeque nasi muscle which originates from the upper frontal process of the maxilla and inserts into the skin of the lateral part of the nostril and upper lip. This slender muscle can be targeted by BTX injected just lateral and inferior to the nasal ala bilaterally (Fig. 57-9). Two to three units of ONA per injection site is all that is required (Fig. 57-10).81

Figure 57-1. Patterns of glabellar injection. By analyzing the patient’s anatomical predisposition, the appropriate number of injection points can be determined. (A) Three injection points. (B) Five injection points.

Figure 57-2. Before and after glabellar treatment. Note reduction of habitually angry expression. (A) Three injection points. (B) Five injection points.
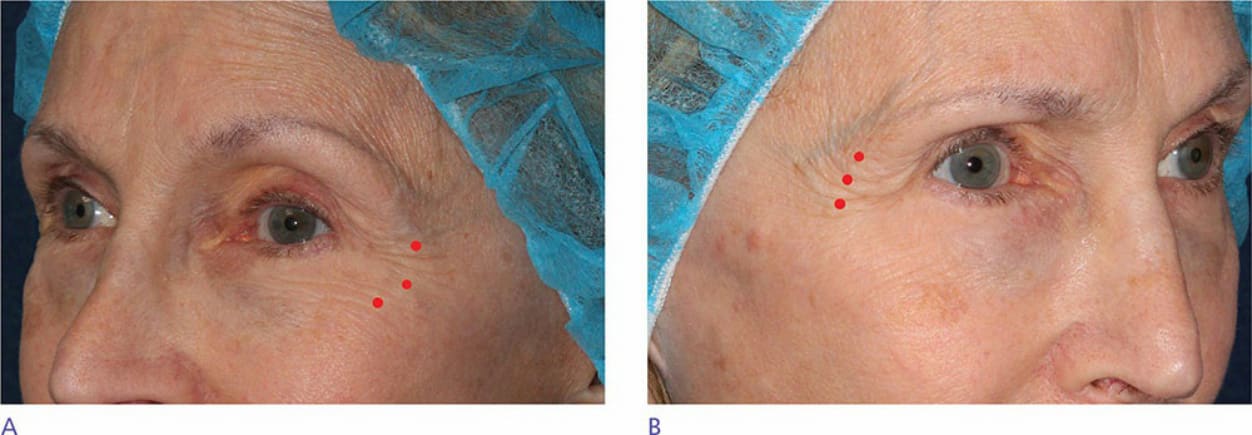
Figure 57-3. Patterns of lateral canthal lines. Different patterns can present in the same individual. (A) Downward fan pattern. (B) Upward fan pattern.
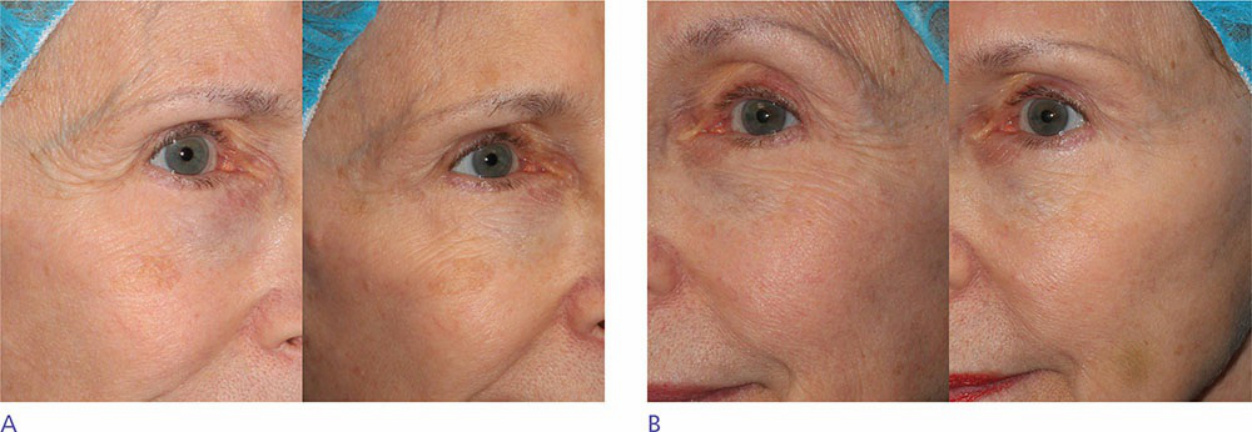
Figure 57-4. Before and after lateral canthal line treatment. Note the relaxation of lateral canthal lines producing a natural, worry-free, and more youthful expression.

Figure 57-5. Frontalis injection. A small number of units should be placed high into the frontalis in order to minimize the chance of inducing brow ptosis.

Figure 57-6. Reduction of horizontal forehead lines. Concomitant treatment of glabella and frontalis is recommended to achieve the optimal cosmetic result.

Figure 57-7. Infraorbital injection. The purpose of this placement is to relax the pretarsal orbicularis oculi, reducing fine lines and leading to a subtly increased palpebral aperture.
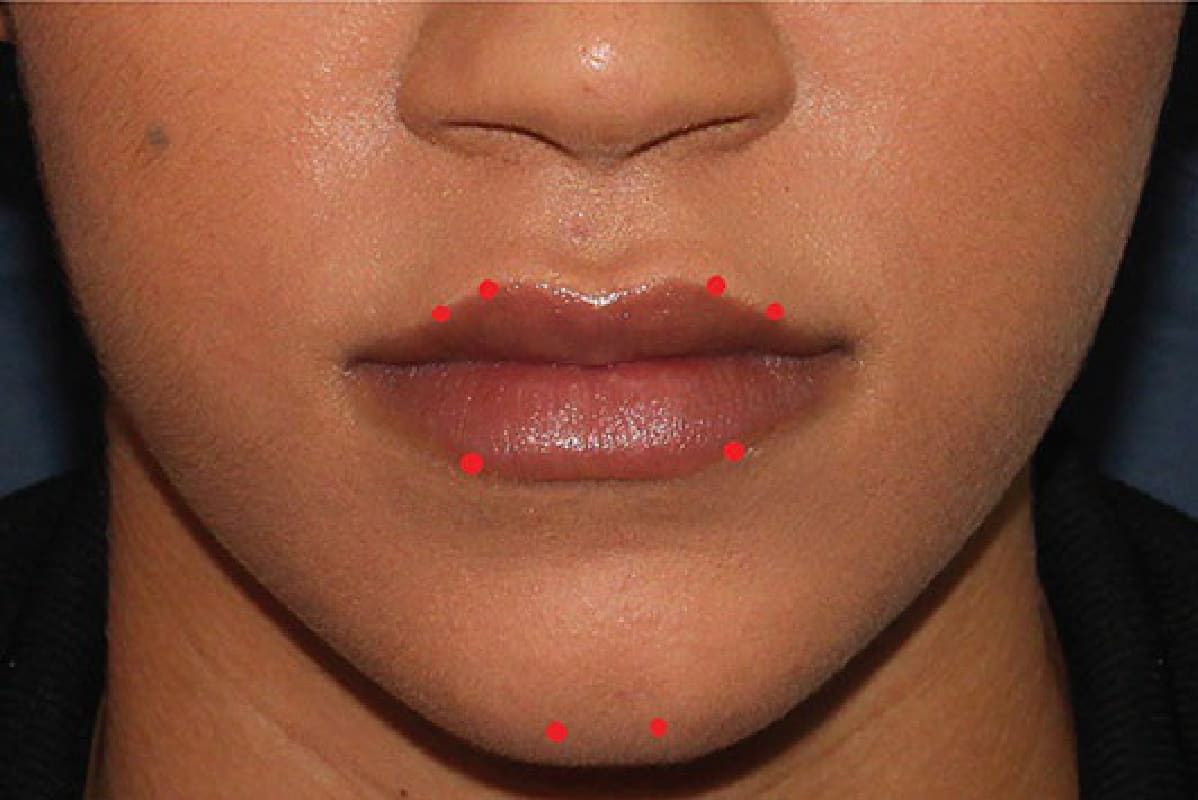
Figure 57-8. Orbicularis oris and mentalis injection.
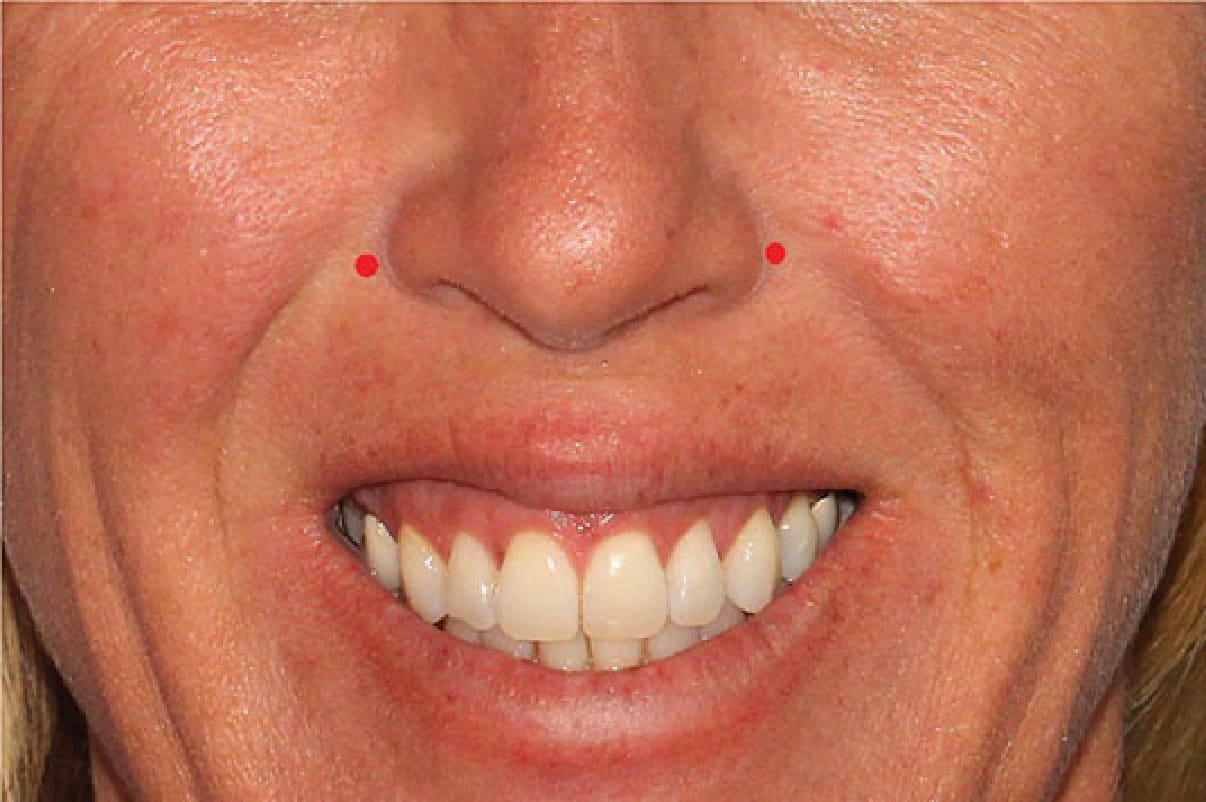
Figure 57-9. Reduction of excessive upper gum show is achieved by targeting the levator labii superioris alaeque nasi muscle.

Figure 57-10. Before and after reduction of excessive upper gum show. Also note the concomitant elimination of the infranasal crease.