Electrobrasion
Electrobrasion
In electrobrasion, an electrosurgical device is used to ablate the skin. The body of the hand piece is held with the thumb and middle finger, while the index finger is used to trigger the electric current. The grip is similar to holding a pen. The device should be set at low to mid power. Higher settings with multiple passes may result in deeper dermal damage than intended.7
Several tips may be used. A smaller, needle point tip is useful for treating fine, small areas. A larger flatter tip can be used to plane down larger areas of tissue, such as in rhinophyma. In electrobrasion of scars, the flat portion of the tip is moved gently across the surface of the skin.8 A sweeping motion is used to paint the treatment area to the level of the papillary or reticular dermis depending on the nature of the scar or tissue irregularities to be treated. Unlike dermabrasion, there is minimal bleeding with electrobrasion, and this cannot be used as a landmark for reaching the papillary dermis.
After the treatment area is completely ablated, one should feather the periphery at lower settings to blend in the surrounding skin for a natural appearance. Postoperative care is similar to dermabrasion.
COMPLICATIONS
To optimize outcomes for patients, an understanding of the potential complications that may result from dermabrasion, and the solutions that can be utilized to prevent or fix these problems, is very helpful (Table 56-6).
One of the most common issues following dermabrasion is the development of a bacterial or viral infection. History of impetigo or herpes simplex infection should be elicited during preoperative evaluation to assess the need for prophylactic treatment. If necessary, cephalexin 1 g daily for 10 to 14 days or valacyclovir 1 g daily for 7 to 14 days can be used for this purpose. Infections of any type can extend the depth of injury and lead to hypertrophic scaring. Patients should be instructed on performing
appropriate dressing changes and educated on how to use dilute vinegar soaks to help prevent infection. If a patient is not able to perform this at home, they should follow up daily in clinic for dressing changes and gentle debridement. Infection will usually manifest as significant pain several days after dermabrasion.
Another common problem following dermabrasion is postinflammatory pigment alteration. Along with wound care, diligent sun protection must be emphasized. The use of tretinoin cream 2 weeks preoperatively has been shown to significantly reduce the incidence of milia and postinflammatory hyperpigmentation.37 Hydroquinone can be used to lighten the skin. It is also essential to have a frank discussion regarding the risks of significant dyspigmentation in patients with darker complexions who are interested in proceeding with dermabrasion.
Scarring following dermabrasion can result from both inadequate treatment of preexisting scar or formation of new scarring. The former problem can be optimized by treating the skin 6 to 8 weeks following injury, as this has been shown to be the optimal time for treatment.22 The risk of scarring increases when dermabrasion is performed deep to the level of the papillary dermis, as this will disrupt the population of stem cells residing around adnexal structures that are necessary for reepithelialization. Bright red erythema 2 to 3 weeks following dermabrasion can be a sign of early scar formation. Intralesional steroid injection and pulsed-dye laser may be used to improve scar outcome (Figs. 56-16 to 56-20).38
CONCLUSIONS
Dermabrasion is an important technique that is used widely in dermatologic surgery. Manual dermabrasion is generally performed in the postoperative period to improve scar appearance, and is particularly well suited to the treatment of flap and graft sites when pincushioning or textural or color mismatch is pronounced. Traditional dermabrasion may be utilized as a full-face approach, though it should always be weighed against the potential role for laser resurfacing or medium depth chemical peels. Electrobrasion is another option that is easy to perform in an office setting and does not require additional instruments; regardless of approach, patients should be warned regarding the potential risk for serious complications in the posttreatment period, and should be highly motivated and educated prior to proceeding with the procedure.
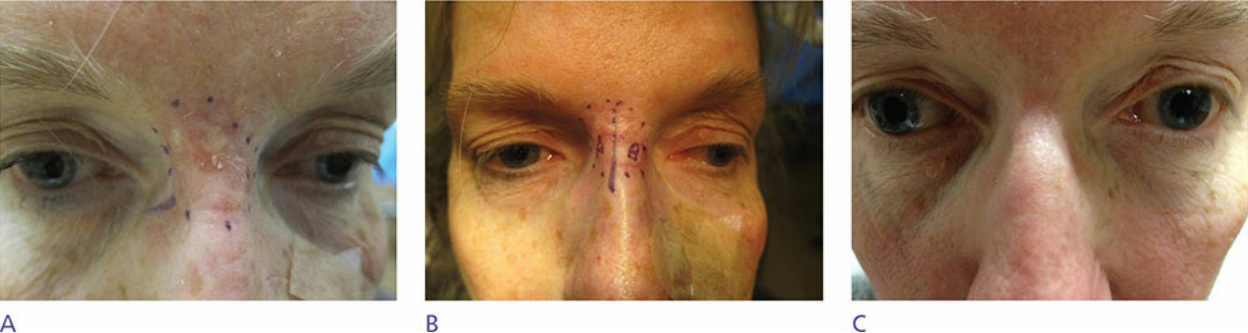
Figure 56-16. (A) Pretreatment scar resulting from full-thickness skin graft following Mohs surgery. (B) Side A randomized to manual dermabrasion and side B randomized to electrobrasion. (C) Follow-up at 3 months following treatment showing improvement in scar with both treatment modalities.
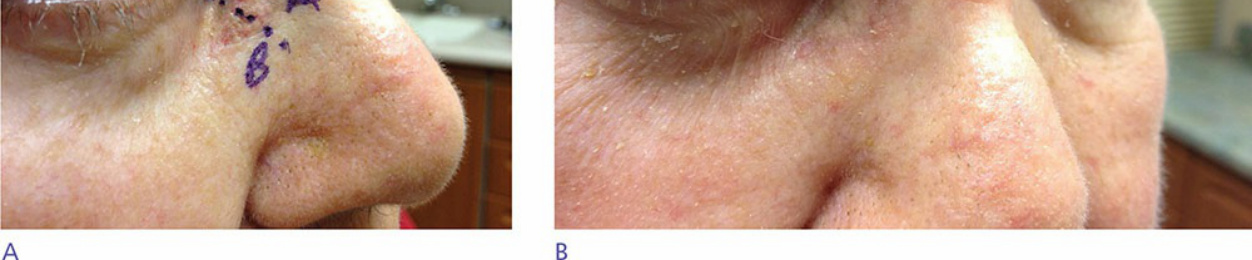
Figure 56-17. (A) Pretreatment scar resulting from full-thickness skin graft following Mohs surgery. Side A randomized to manual dermabrasion and side B randomized to electrobrasion. (B) Follow-up at 3 months following treatment showing limited improvement in scar with both treatment modalities.

Figure 56-18. (A) Pretreatment scar resulting from full-thickness skin graft following Mohs surgery. Side A randomized to manual dermabrasion and side B randomized to electrobrasion. (B) Follow-up at 3 months following treatment showing limited improvement in scar with both treatment modalities.
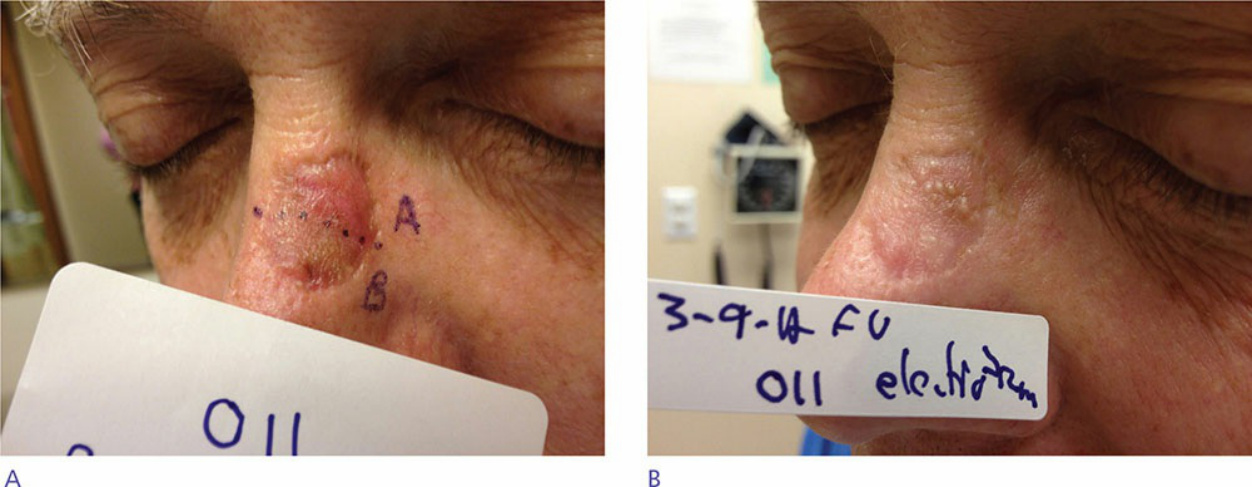
Figure 56-19. (A) Pretreatment scar resulting from full-thickness skin graft following Mohs surgery. Side A randomized to manual dermabrasion and side B randomized to electrobrasion. (B) Follow-up at 3 months following treatment. Note development of milia in side treated with dermabrasion.
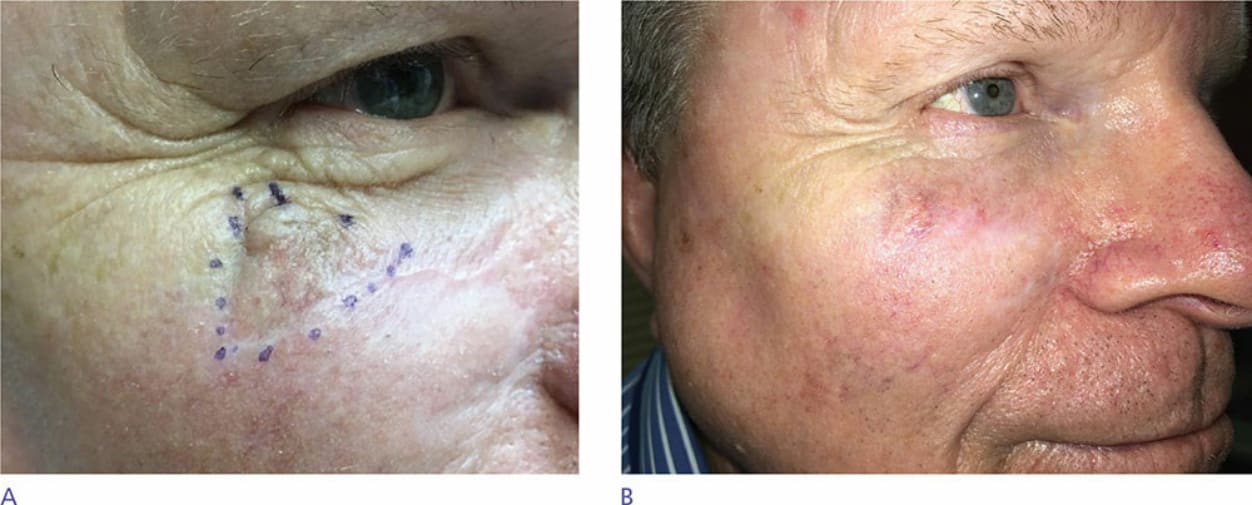
Figure 56-20. (A) Pretreatment scar resulting from advancement flap following Mohs surgery. (B) Follow-up at 3 months following treatment with electrobrasion.
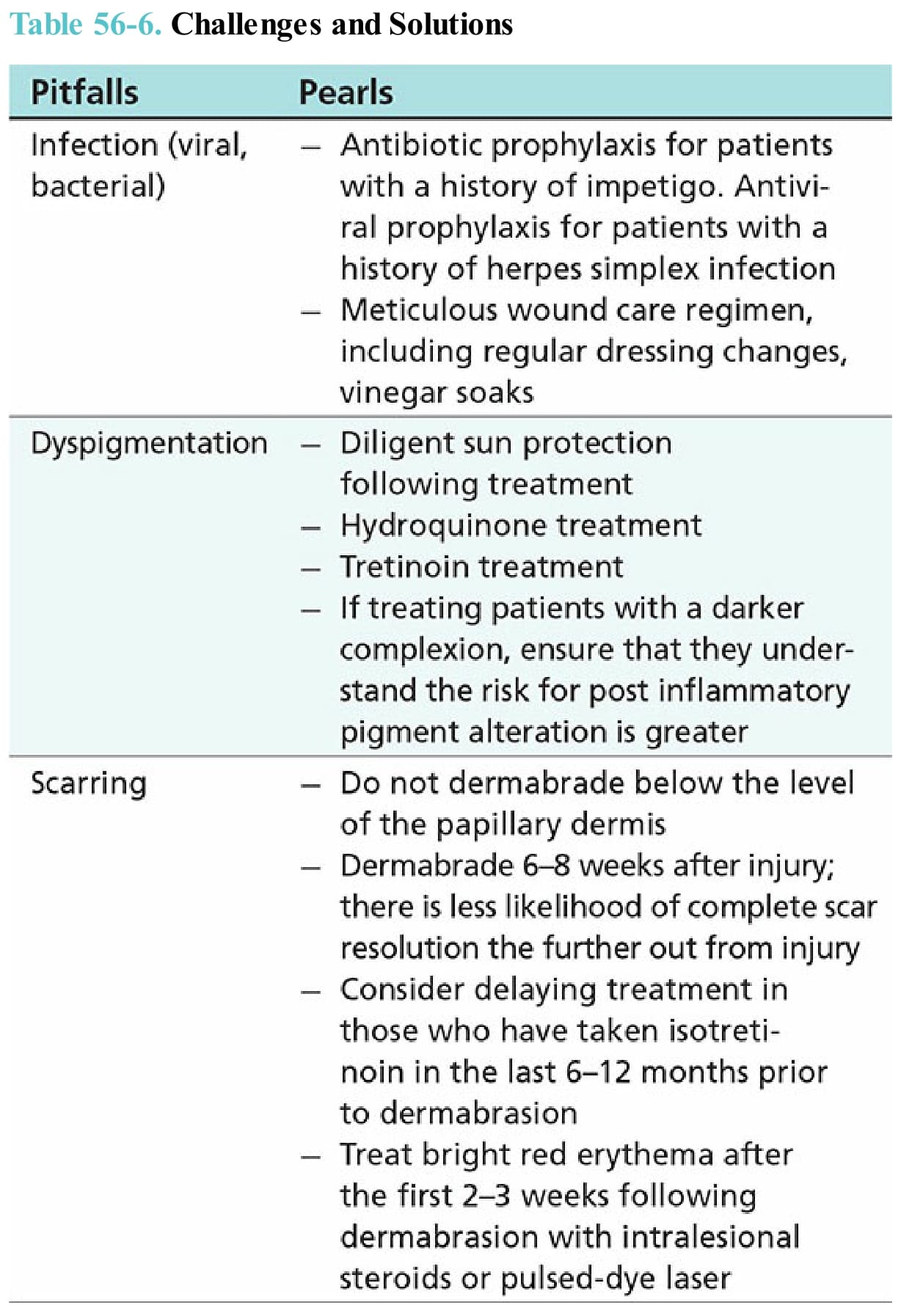
Table 56-6. Challenges and Solutions