ADDITIONAL SURGICAL CONSIDERATIONS
ADDITIONAL SURGICAL CONSIDERATIONS
Surgery is the cornerstone of HS treatment and may achieve local cure. However, the surgical treatment can be complex.
Preoperative assessment to identify nodules and sinus tracts is primarily done by inspection and palpation. However, the extent of the sinus tract formation can only be established during surgery, and the affected area is often considerably larger than expected based on the preoperative assessment. The addition of color Doppler ultrasound may add relevant information prior to surgery. Ultrasound examination, when performed by a skilled radiologist or dermatologist with experience in skin imaging, can give insight into the exact location, number, and size of the sinus tracts.48 This may help to achieve a more anatomically oriented and precise excision.
Second, even though healing by secondary intention is the preferred method, some areas, specifically the buttocks, benefit from a shorter healing time. The suggested closure technique for this location is with an STSG (Fig. 54-12A, B, C). STSGs are traditionally taken from a donor site outside of the affected area, often from the upper leg. As HS originates from the hair follicles and the epidermis is healthy, a thin STSG could also be harvested from the HS-affected area selected for excision. This reduces the burden on the patient as there is no donor site wound and cosmetically undesirable scar from the donor site. The STSG can be harvested using an electric or air-driven dermatome, set to cut at a thickness of 0.2 to 0.3 mm. After harvesting the STSG is meshed in a 1:1.5 ratio. Storing the STSG wrapped in a saline-moistened gauze in a refrigerator at 4°C allows for delayed grafting. Delayed grafting is necessary, as the depth of the excision in HS should reach the healthy subcutaneous fat which cannot sustain skin grafts. After approximately 14 days, the granulation tissue is developed properly and will support STSG. The use of platelet-rich plasma (PRP) increases the chance of survival of the STSG and forms a protective layer fixing the STSG in place without the use of glue or staples. First, half of the PRP should be applied to the
granulating wound bed. The residual PRP should be applied on top of the STSG and activated by calcium- containing autologous serum, resulting in entrapment of the STSG in a thrombin-fibrin gel which ensures firm adherence to the wound bed.
Last, photodynamic therapy (PDT) may be useful in the treatment of HS through selective, cytotoxic, and immunomodulatory effects.49 Patients with long-standing HS sinus tracts unwilling or unable to undergo excisional surgery may benefit from a less invasive treatment with intralesional PDT. The procedure starts with administration of a local anesthetic, preferably using bupivacaine to prolong the anesthetic effect, followed by filling the sinus with a photosensitizing 5% 5-aminolaevulinic acid (5-ALA) gel using a plastic cannula.50 During the incubation period of approximately 2 hours, the inlet/outlet needs to be covered in order to keep the photosensitizing solution within the cavity and in the dark. Subsequently the tip of an optical fiber at 630 nm is inserted in the opening until the end of the sinus tract is reached. Next, the cavity is irradiated by a laser in continuous mode at 1.2 W while slowly retracting the fiber.50 A prospective case series treating HS patients with intralesional PDT demonstrated a 76% (29/38)
complete response.50 Best results are obtained in single or isolated sinuses. In patients with multiple, interconnected, or deep sinuses, two or more sessions are more frequently needed to achieve maximum response. Follow-up sessions can be performed at intervals of 5 to 7 weeks.
Patients with HS in the perianal or perineal area, especially male patients and those with concomitant intestinal bowel disease (IBD), are at risk of developing sinus tracts penetrating through the anal sphincter complex or communicating with the rectum (i.e., fistulas).51 Moreover, recent investigation showed that the prevalence of IBD in HS patients is four to eight times higher compared with the general population (3.3% vs. 0.41–0.74%).51 The presence of trans- or intersphincteric sinuses or fistulas should preferably be assessed by endorectal coil MRI preoperatively. Alternatively, a fistulogram could be performed. Patients with trans- or intersphincteric sinuses or fistulas should be operated on in collaboration with a gastrointestinal surgeon, who can insert a seton to mark the fistula or sinus tract.52
Secondary intention healing is the preferred management for excisions in HS. Theoretically secondary intention healing may reduce the rate of recurrence by allowing the remaining aberrant keratinocytes or residual keratin fibers to escape from the wound. Trapping these remnant foci of disease by primary closure or re-introduction of hair follicles in a site of HS predilection by flap reconstruction may induce recurrence in the operated area. However, to date there is no literature available to support this hypothesis.
CONCLUSIONS
Surgery is indicated throughout all stages of HS, with the exception of the mildest forms (Fig. 54-13). Acute surgical interventions, that is, intralesional injection of triamcinolone and incision and drainage, can be performed to quickly relieve symptoms of inflammatory nodules and tense abscesses. For these procedures cryoanesthesia is preferred. Local cure of HS can be accomplished with elective surgical procedures. Smaller areas can be treated with deroofing and/or limited excision, depending on the presence of epithelialized cavities. For affected areas of at least 1% (Hurley III) a wide excision is indicated. Healing by secondary intention is preferred over primary closure, as the latter could trap remnant (active) foci of disease underneath the skin, resulting in recurrence. Special attention should be paid to the possible presence of trans- or intersphincteric sinuses or fistulas in patients with perianal/perineal HS. To ensure the best patient outcomes, surgeons should select the appropriate surgical technique based upon operator experience and the individual needs of the patient.

Figure 54-12. Course of wound healing with the use of split-thickness skin grafts and platelet rich plasma. (A) Hurley III on buttocks before wide excision. (B) Delayed application of STSG 14 days after wide excision. (C) Result 48 days after surgery.
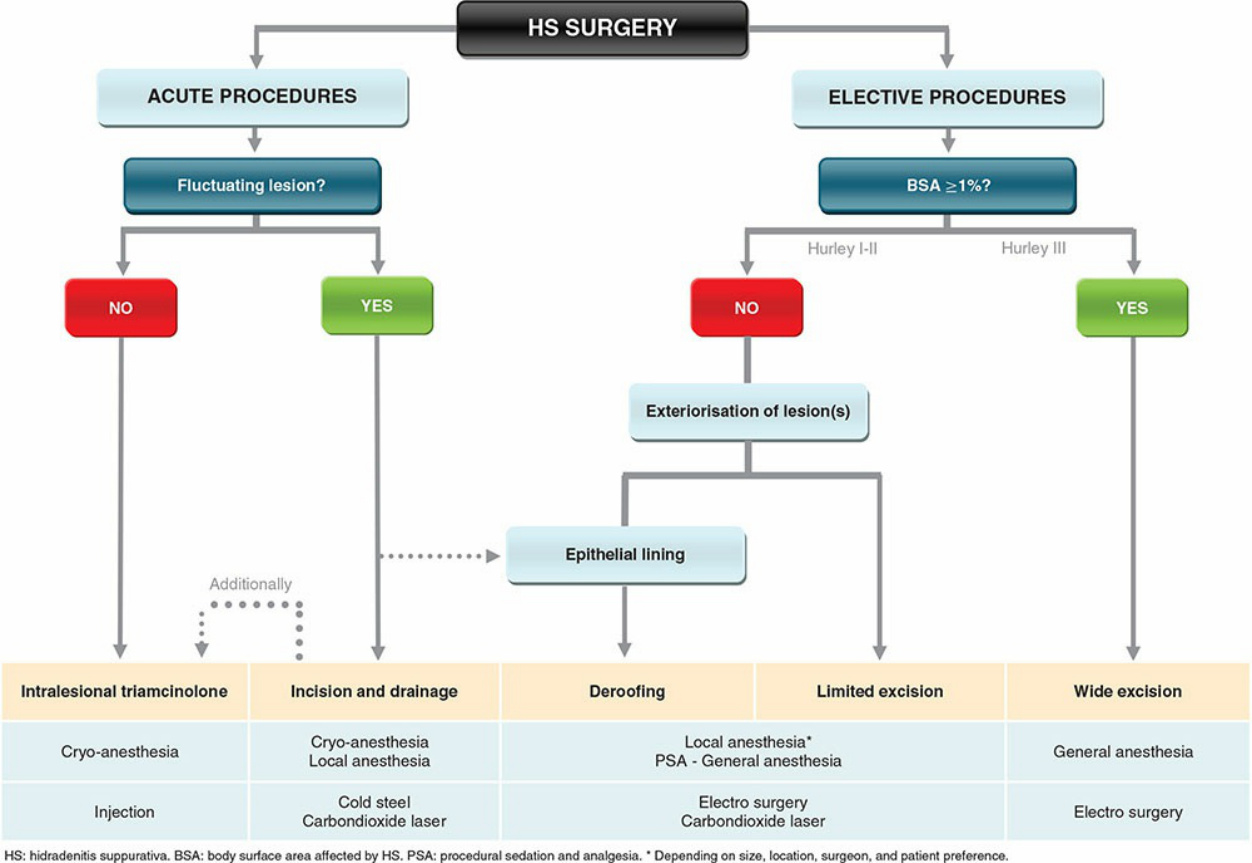
Figure 54-13. Schematic overview of surgical treatment algorithm.