Techniques
Techniques
Most of the steps in the wide excision procedure are similar to those of the limited excision. However, in contrast to a limited excision, electrosurgery is preferred over evaporation by CO2 laser in these large areas (≥1% BSA). Injection of a 1% methylviolet or methylene blue solution into the sinus tracts may be considered to ease the localization of sinus tracts during the procedure.34 The epidermis, its appendages, sinuses, and associated inflammation and scar tissue should be removed only until soft, normal-appearing subcutaneous fat remains, taking into account a surgical margin up to 1.0 cm. Wide excision does not require the destructive en bloc deep to the fascia technique used in managing malignancy.17 In addition, the affected area should be excised in multiple stages during the procedure. This will result in a better overview and allows for better localization of additional sinus tracts as the often profuse bleeding can be more easily contained. When the affected area is totally removed, the edges are carefully palpated and probed to check for additional sinus tracts or cavities (Fig. 54- 10A and B).
After removal of extensive HS lesions, there are multiple options for wound healing or reconstruction. Healing by secondary intention is preferred even for large defects, as minor residual foci of disease are allowed to migrate to the surface and may spontaneously heal. However, wound reconstruction may accelerate the healing of
postsurgical skin defects and thus prevent the prolonged healing time associated with secondary intention healing. Several techniques have been described to close large defects after wide excision.38 Primary closure with flap reconstruction (e.g., local, rotation, or transposition) should best be avoided because the reintroduction of hair follicles in a site of HS predilection may result in recurrence within the flap (Fig. 54- 11). For defects where shorter healing time is preferred, such as defects on the buttocks, an alternative closure technique is the use of autologous delayed split-thickness skin grafting (STSG) and platelet-rich plasma.45 It is a relatively easy, inexpensive procedure which reduces postoperative morbidity and pain and may accelerate recovery after extensive HS surgery.
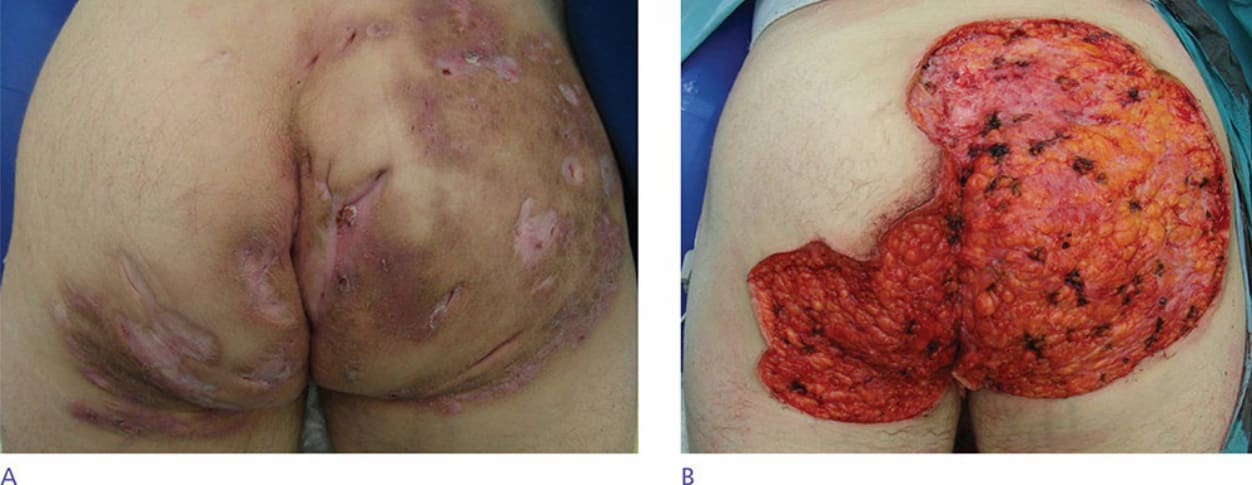
Figure 54-10. (A) Hurley III of the buttocks before wide excision. (B) Result directly after wide excision.

Figure 54-11. Recurrence in transposition flap in the left axilla.