Electrosurgery
Electrosurgery
The skin is disinfected using a chlorhexidine, povidone iodine, or 70% ethanol solution (which needs to evaporate completely before starting the procedure). First, the affected area is palpated thoroughly to estimate the extent of the excision. The anticipated area can then be outlined using a marker (incorporating a ~0.5-cm margin). The subsequent electrosurgical incision is performed using a blade or needle electrode tip at 35 W in cutting mode (major surgery setting). Dissection of the affected skin from the subcutaneous fat can be performed using the “cut” or “coagulation” mode. Performing the dissection in coagulation mode will result in less bleeding, but the tip may have more difficulty moving through the tissue. A practical tip is to keep the skin stretched under traction to facilitate dissection.34 Subsequently, the edges are palpated and probed in search of additional sinus tracts. Once the area is clear of lesions and there is no further bleeding, the wounds are left open for secondary intention healing.
Carbon dioxide laser vaporization A CO2 laser with a wavelength of 10,600 nm is an effective alternative to electrosurgery in the treatment of HS.35 This technique minimally affects the surrounding tissue and offers increased visualization of the operative site by partial hemostasis.17,36,37 First, if possible, a blunt probe is used to identify separate or interconnected tracts. The laser is used in continuous-wave mode at 20 to 30 W, generally with a spot size of 3 mm, to evaporate gradually top-down both superficial and deeper lesions. Second, layers of the affected skin including the proliferative gelatinous mass are vaporized by repeated passes of the laser until healthy tissue is reached (Fig. 54-8A and B).36,37
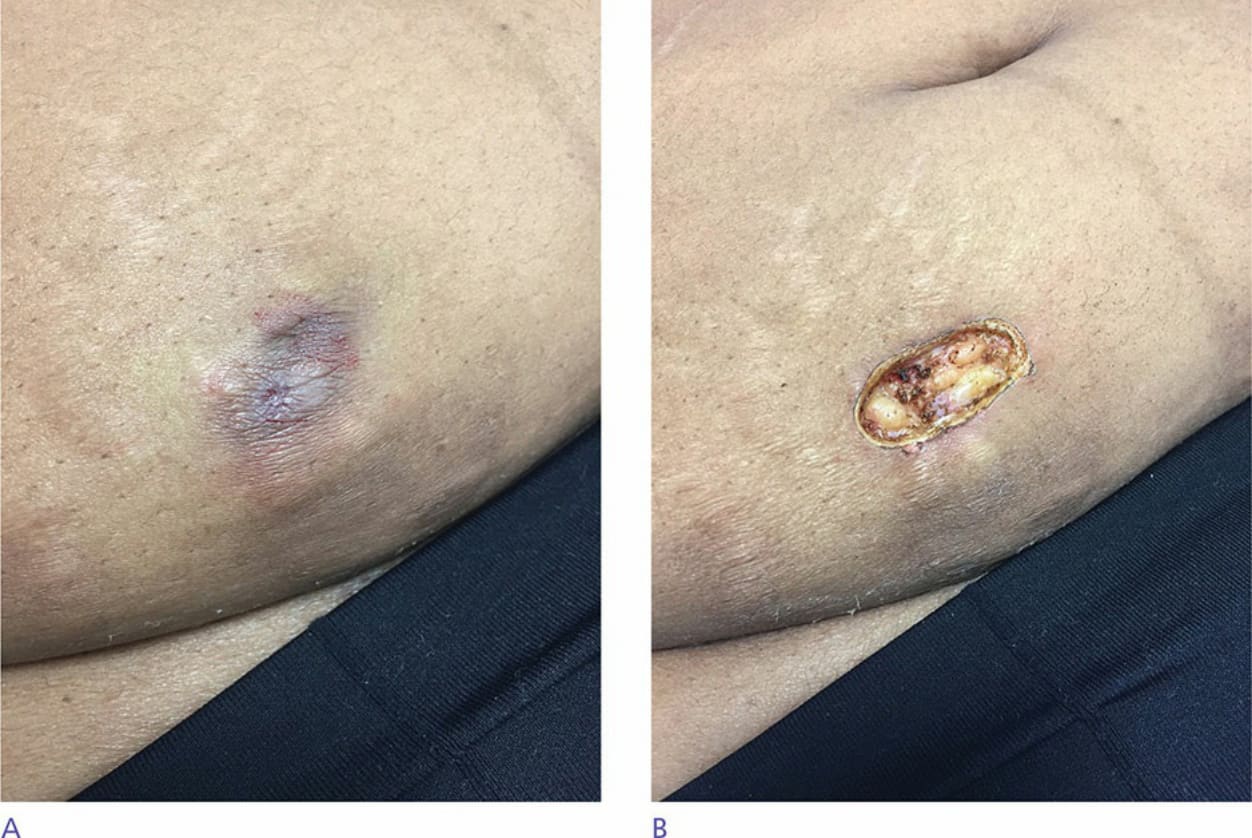
Figure 54-8. (A) Solitary nodule before CO2 laser destruction. (B) Result directly after CO2 laser destruction.