Technique
Technique
HS lesions selected for deroofing are identified by visual inspection and palpation, and can subsequently be marked with ink.25 After visual inspection and palpation, a blunt probe is inserted in a sinus opening (Fig. 54-6A). When a probe is not available, the blunt tip of a closed, fine forceps or “mosquito” could be used. In case no openings are detected, a small incision is made to introduce the probe. An incision is made over or around the probe using an electrosurgical device in cutting mode or with a CO2 laser. The cavity is subsequently examined with the probe in all directions to find and explore all possible communicating tracts. Sinus tracts can run for long distances dissecting and undermining the dermal layer of the skin. Care needs to be taken not to create false passages. The roof of the lesion must be completely exteriorized from each tract. The inflammatory granulation tissue, recognizable as a gelatinous mass, and reactive fibrosis trapped beneath the surface, must be surgically removed. Although the literature is inconsistent, removing the floor with a curette or electrocoagulation is not recommended.17,25,30 Any residual epithelialized sinus floor—if the surgeon is certain there is no active disease beneath it—is left in situ to assist healing by secondary intention (Fig. 54-6B). Primary closure needs to be avoided because remnant (active) foci of disease could be trapped underneath the skin, resulting in recurrence.
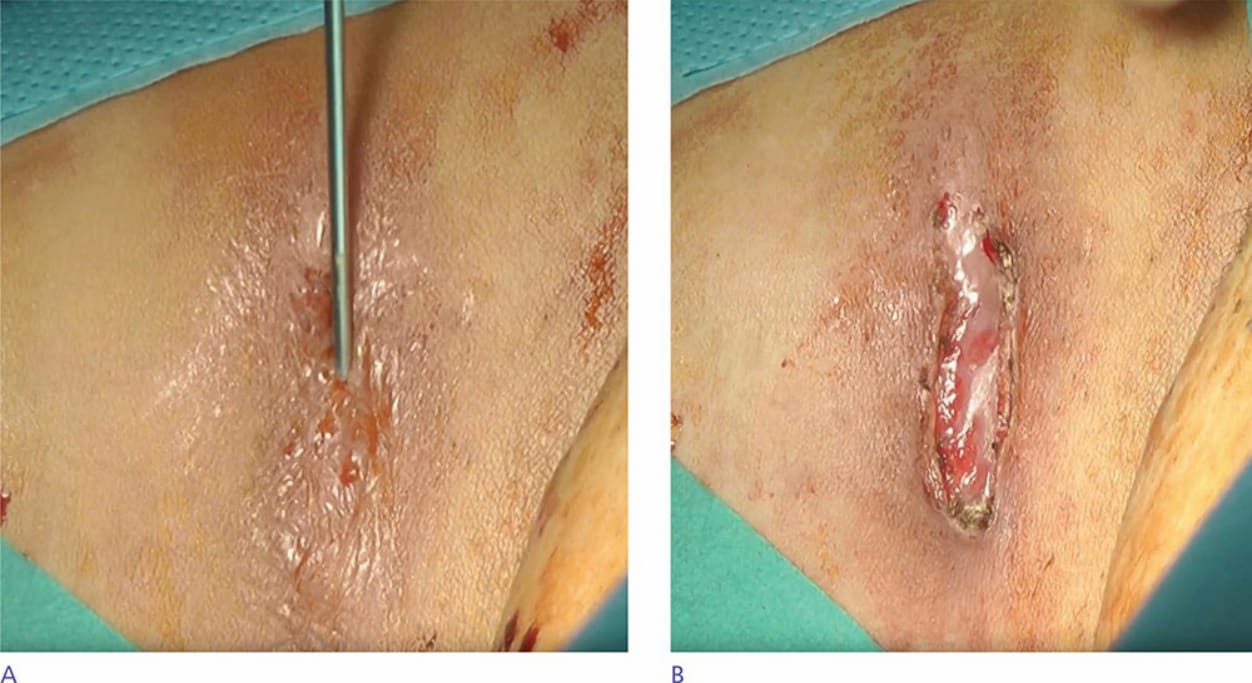
Figure 54-6. (A) Probe inserted in the draining HS lesion in the groin. (B) HS lesion showing epithelialized floor after deroofing procedure. (Used with permission from J. Boer, MD, PhD).