Surgical debridement
Surgical debridement
Surgical or sharp debridement involves the removal of devitalized tissue using sharp instruments such as scalpels, curettes, scissors, and forceps. This procedure may be
performed in an office setting, though select extensive cases may be better suited for the operating room (Fig. 53-1). Surgical debridement is fast and selective, permitting the removal of unhealthy, necrotic tissue while leaving viable tissue intact. It also offers the advantage of accurate assessment of wound size and depth and the presence of tunneling and undermining.7 Excision of the overlying nonviable tissue also allows for the attainment of deep tissue biopsy specimens for culture and sensitivity, and the clinical identification of osteomyelitis, which can be present in as many as 85% of cases with positive probing to bone.16,17 An adequate vascular supply is required for a successful procedure.
Surgical debridement is included in multiple algorithms for the treatment of chronic wounds, though sound evidence for its success is lacking. Treatment guidelines for diabetic foot ulcers (DFUs), for example, include surgical debridement as part of their standard of care.18 In addition to necrotic tissue excision, removal of callus at each visit reduces plantar pressure and sheer forces that may perpetuate ulcer development.9 A secondary analysis from a randomized controlled trial comparing topically applied recombinant human platelet-derived growth (rhPDGF) and vehicle (placebo) in patients with DFUs showed higher healing rates in centers that had higher debridement rates.19
In a prospective study by Williams et al., 55 patients with recalcitrant chronic venous leg ulcers (VLUs) were enrolled to evaluate the effect of sharp debridement on the progression of their wounds over a 12-month period. At 4 and 20 weeks postdebridement, there was a statistically significant reduction in mean surface area in the debridement group and a higher rate of complete healing when compared to patients who did not undergo debridement.20
A retrospective study to determine a correlation between serial debridement of DFUs and VLUs and healing outcomes was performed based on the results of two prospective randomized controlled trials investigating the effects of novel topical
wound treatments. This showed a statistically significantly greater median reduction in wound surface area in debrided VLUs as compared to VLUs without debridement, and centers with more frequent debridement had statistically significantly higher rates of wound closure in both the DFU and VLU study.21 Still, more research is needed, as most existing studies are not randomized controlled trials.
Indications Surgical debridement is indicated for medically stable patients who have wounds with an adequate blood supply.22 Surgical debridement should be considered over other less aggressive forms of debridement if larger amounts of necrotic tissue or thick, adherent eschar are present. It is also indicated to quickly remove tissue in urgent cases, such as in settings of an infected wound, necrotizing fasciitis, or sepsis.6,16
Contraindications Wounds with inadequate circulation should not be debrided, as removal of bleeding tissue in these cases is contraindicated.22 Surgical debridement should be avoided in patients with vascular insufficiency, such as ischemic limbs, and in stable, poorly perfused heel ulcers, unless infection is suspected.6,23 Debridement of wounds due to pyoderma gangrenosum is also contraindicated due to pathergy, leading to induction and exacerbation of existing ulcers with trauma.24 Debridement should be performed with caution in the setting of clotting disorders or anticoagulants use.6
Technique Office-based surgical debridement requires the use of sharp surgical instruments including forceps, scalpels, curettes, and scissors. Toothed forceps are useful, as they permit the grasping of necrotic tissue while minimizing trauma to normal skin. A number 10, 15, or 21 blade scalpel may be used to remove thin layers of unwanted tissue until reaching a healthy, well-perfused base. Scalpel blades may need to be replaced during the procedure. Sharp scissors are also useful for dissecting and excising thick eschar and necrotic tissue. Curettes work well for removing proteinaceous slough, typically yellow to brown in color and filled with bacteria and proteases that accumulate over the wound bed.7,25
Except in patients with significant neuropathy, premedication with a topical or local anesthetic may be required. Lidocaine-prilocaine cream (euctectic mixture of local anesthetics [EMLA]; AstraZeneca, Wilmington, DE) is the only evidence-based topical anesthetic indicated for debridement of lower extremity ulcers. In randomized controlled trials, EMLA led not only to improved pain control in leg ulcers, but also aided mechanical debridement as measured by shortened time to a clean ulcer.26–29 It should be applied at least 20 minutes prior to debridement to achieve analgesia.7 For
more aggressive in-office debridement, a ring block with lidocaine is another option.25
The goal of debridement is to obtain a clean, well-vascularized wound bed, transforming a chronic wound into an acute wound capable of progressing through the phases of healing normally.30 In chronic wounds, only nonviable, nonbleeding tissue should be removed,22 which is often brown or black in color.7 It is sometimes clearly demarcated from viable tissue and can be dissected along that line of demarcation. If unable to clearly distinguish healthy from devitalized tissue grossly, thin sections of tissue should be excised until reaching clearly viable tissue. Viable tissue should demonstrate punctate bleeding and no clotted venules along the wound edge.25
There is no clear guideline on the extent to which a wound should be debrided, though nonhealing edges of wounds have distinctly different gene expression profiles than viable adjacent skin.15 For successful debridement, the excision must include a margin of response of cells that are healthy enough to respond to wound healing stimuli.31 Saap and Falanga developed a Debridement Performance Index to determine the adequacy of debridement of DFUs. This scoring system was found to be an independent predictor of wound closure in their study, including the presence of callus, undermining, and wound bed necrotic tissue as scoring parameters.32 The same researchers later developed a Wound Bed Scoring System using healing edges, presence of eschar, greatest wound depth/granulation tissue, amount of exudate, edema, periwound dermatitis, periwound callus and/or fibrosis, and a pink/red wound bed as parameters. Higher scores correlated with better healing outcomes.33
Complications and limitations As with any operative procedure, there is risk of introducing infection and the expansion of a nonhealing ulcer. Intolerable pain may complicate surgical debridement, and such cases may be better suited for management in the operating room under general anesthesia.25 In cases with a large wound surface area, bedside debridement may be inappropriate due to inability to assure anesthesia and the risk of uncontrollable bleeding, and should be reserved for the operative setting for better hemostatic control. Bedside debridement is also inappropriate for cases where debridement of deeper structures such as tendons, bone and vascular structures are involved, and in cases where emergent surgery is required, such as with sepsis.30
Follow-up care Improvement following debridement may not be apparent until 2 to 4 weeks postoperatively. However, debridement is typically not a one-time event, as many wounds require repeated debridement to maintain a wound environment conducive to healing.6 One study showed greater healing rates were associated with higher debridement rates,19 while another study demonstrated no statistically significant
correlation between frequency of debridement and higher rates of wound closure, though there was some evidence of a beneficial effect in DFUs.21 Wilcox et al. performed a recent retrospective cohort study with the largest data set to date, including 154,644 patients with 312,744 wounds of all causes, to investigate healing outcomes with debridement frequency. The results showed that frequent debridement was associated with shorter healing time.34 In a retrospective cohort study by Warriner et al., more frequent visits and sequential debridement translated into increased healing, lower costs, and better quality of life for patients with DFUs and VLUs.35 In general, an Unna boot or other compressive approach is required for any treatment for lower extremity chronic wounds (Fig. 53-2).
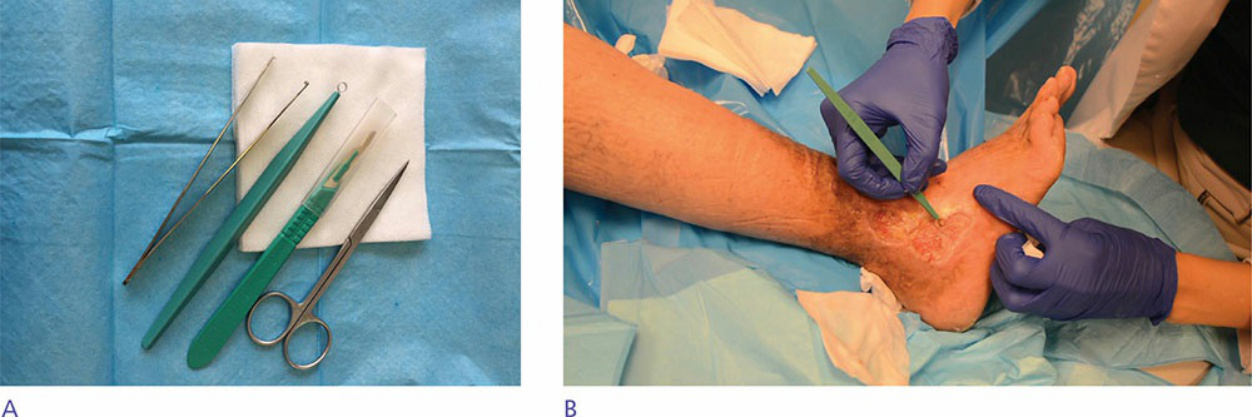
Figure 53-1. Debridement is a straightforward approach to chronic wound care. (A) A simple set of instruments may be used for debridement, including forceps, curette, scalpel, and scissors. (B) Curettage of necrotic and devitalized tissue may be performed both over the center of the wound and around the wound edges.

Figure 53-2. Unna boot placement step-by-step. (A) A specialized Unna boot and cohesive bandage may be used for placement. (B) and (C) The first layer is placed using a loose overwrap technique that permits gentle coverage without compression. (D) At this point the entire lower extremity is covered with the first layer. (E) The cohesive bandage is then wrapped over the dressing and (F) a final layer of compression is then placed.