Cryosurgery
Cryosurgery
Cryosurgery is a minimally invasive ablative technique that uses a cryogen to destroy tissue by rapid freezing followed by a slow, prolonged thaw. Cryosurgery is a simple, fast, and inexpensive approach to NMSC management, and is most appropriate for treating small discrete primary lesions such as superficial BCC and SCC in situ. Cryosurgery is particularly beneficial in patients with multiple NMSCs, as multiple lesions may be treated in a short period of time during a single office visit. This approach may be used safely in patients with complex medical conditions, though the ease of the procedure must be weighed against a possible extensive healing process. Moreover, cryosurgery does not provide any specimen for pathological examination. Treatment should include a 2- to 5-mm margin of normal appearing tissue to ensure adequate treatment.
The magnitude of destruction is a function of temperature, application pressure, and exposure time. Destruction of malignant cells requires temperatures between –40oC and
–60oC. Liquid nitrogen (LN2) is the most commonly used cryogen in dermatologic surgery as its low temperature (–195.8°C) ensures the possibility of tissue destruction. The molecular basis for cryosurgery is multifactorial in nature (Table 48-1), involving direct cell injury during the initial freeze and mechanical destruction and crystallization of the cell wall leading to membrane instability and cell lysis.18 During the thaw portion of treatment, vascular injury occurs. Intense vasoconstriction during the freeze cycle changes vessel wall permeability, and when blood flow resumes during the thaw, compensatory hyperperfusion leads to free radical damage and membrane oxidation with ensuing ischemia.19 These mechanisms of injury lead to apoptosis even in regions where the temperature was not sufficiently low to lead to direct cell necrosis; in addition, an intense T-cell immunologic response occurs, further inhibiting tumor growth.20–22
The cryogen delivery unit must accurately and reproducibly achieve temperatures capable of eliciting cell death at the deep and lateral margins of the lesion. There are four central cryogen delivery techniques for cryosurgery to the skin:23
Open spray: LN2 is delivered through the open end of the cryogen delivery unit. Spray
tips are available with different apertures to allow for treatment of different sized lesions. Larger nozzles freeze more quickly, leading to a greater but less precise area of destruction.
Confined spray cones: This variant of the open spray technique uses a circumscribed
cone on a plastic plate to concentrate the spray on a specific area. This also reduces inadvertent tissue destruction or splashing of LN2.
Chamber or closed-cone: A metal cylinder with an open rubber-covered base is firmly
applied to the target tissue to help achieve a deep freeze.
Closed system or probe: Cryoprobes are metal devices used to make direct contact for
cryosurgery. This allows for direct contact and delivery of LN2 through the probe. It is ideal for lesions in hard to reach areas with a flat surface.
Once the proper delivery device is chosen, the area is frozen by delivering LN2 to the affected area in a controlled manner. It is then allowed to thaw for 60 to 120 seconds to return to the original skin temperature. Since much of the vascular injury
occurs during the reperfusion of the thaw cycle, it is imperative to allow complete thawing before repeating the freeze–thaw cycles. The optimal number of freeze–thaw cycles to adequately treat NMSC has not been determined. For very superficial NMSC, one cycle may be appropriate, though at least two cycles should be performed for thicker lesions. Studies suggest that the second freeze–thaw cycle increases the extent of original necrosis by 80%, significantly decreasing the risk of partial or inadequate treatment (Fig. 48-4).24
Cryosurgery is typically reserved for BCC, well-differentiated SCC, and SCC in situ. Cure rates for cryosurgery at 5 years postprocedure have been reported as 93% and 96% for low-risk BCC and SCC, respectively, though like EDC it has not been rigorously studied in a randomized controlled trial setting.25–27 Its advantages include ease, speed, and low cost. Disadvantages are similar to EDC and include prolonged healing duration (which may last 4–6 weeks), pain and edema at the site, postoperative bullae formation, and associated hypopigmentation. Future use of optical coherence tomography and confocal microscopy28,29 may augment the reliability of cryosurgery, which may then be used as an adjuvant approach to minimize tumor recurrence.

Figure 48-4. Elliptical surgical excision of a nonmelanoma skin cancer.
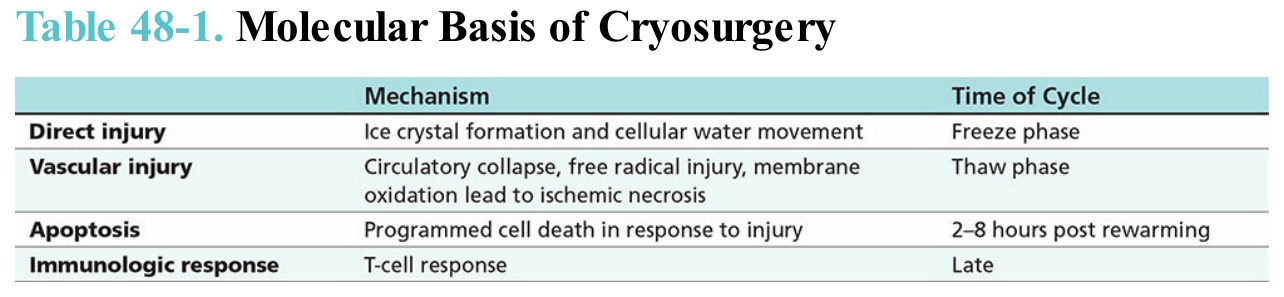
Table 48-1. Molecular Basis of Cryosurgery