Deciding when to reexcise DN
Deciding when to reexcise DN
Despite the intent to perform an excisional biopsy of a pigmented lesion, histologically positive margins can be left behind. By definition, a histologically positive margin is expected in a partial incisional biopsy. The NIH consensus paper on DN from 1992 had no guidelines on reexcision of DN, and clinicians have had the challenge of determining when to recommend a reexcision after an initial biopsy of DN.9 The decision to perform reexcisions for DN has been variable geographically as there is a paucity of data to help understand the actual risk of transformation of melanoma from DN. In 2002, a survey of members of the AAD revealed that 67% of respondents preferred to reexcise DN with a positive histologic margin.56 However, several recent studies published have examined the role of observation for DN with positive histologic margins.84 In addition, studies
by Goodson et al. and Hocker et al. also observed a combined total of 184 DN with positive histologic margins, and no melanomas eventuated from the biopsy sites with greater than 2 years and an average of 17.4 years of follow-up, respectively.81,85 Two additional studies examined a total of 219 reexcisions of DN with positive histologic margins to assess for presence of melanoma in the reexcision specimen.86,87 While the study by Abello-Poblete found no melanomas within the reexcision of DN with positive histologic margins, the study by Reddy et al. found that 2 out of 127 reexcisions (1.6%) revealed melanoma in situ arising from initial lesions biopsied and diagnosed as moderately to severely DN, and the authors suggested reexcisions for higher-grade DN with positive histologic margins. More recently, a study of 498 patients with mild or moderate DN with positive margins at biopsy demonstrated a very low rate of conversion to melanoma, with 2% of observed DN demonstrating conversion to melanoma versus 0.06% or reexcised DN.88 Though this difference was not statistically significant, the study may not have been powered to detect such a small effect size and therefore careful consideration of reexcision should continue.
Recent studies have shown that over time, more clinicians choose clinical observation for lower-grade DN with positive histologic margins. A 2009 survey of Chicago dermatologists revealed that while 79% of respondents observed mildly DN with positive margins, 81% reexcised moderately DN with positive margins, and 95% reexcised severely DN.19 In a 2014 survey of New England dermatologists on management of DN with positive margins and no clinical residual pigment, 95% of respondents observed mildly DN with positive histologic margins, while 39% observed moderately DN with positive margins, and 100% reexcised severely DN (see Table 47- 5).89 Most dermatologists agree that severe DN with a positive margin should be reexcised because of the possibility that these lesions may overlap histologically with early melanoma.56,89
To highlight the clinical gap in recommendations for management of biopsied DN with positive margins, the Pigmented Lesion Subcommittee of the Melanoma Prevention Working Group published a consensus statement in 2015, and through the Delphi technique of consensus building, recommendations about management of DN with positive histologic margins were suggested by the authors.2 Included in the recommendations was the consensus that DN with mild or moderate atypia and clear histologic margins do not need to be reexcised. Also, mildly DN with a positive histologic margin and no clinical residual pigmentation can be managed with observation. For moderately DN with positive histologic margins and no clinical residual pigmentation, the consensus statement recommended that clinical observation may be appropriate, though more data are needed. There was consensus that all severe DN with positive histologic margins should be reexcised to achieve a 2- to 5-mm clinically free margin.90
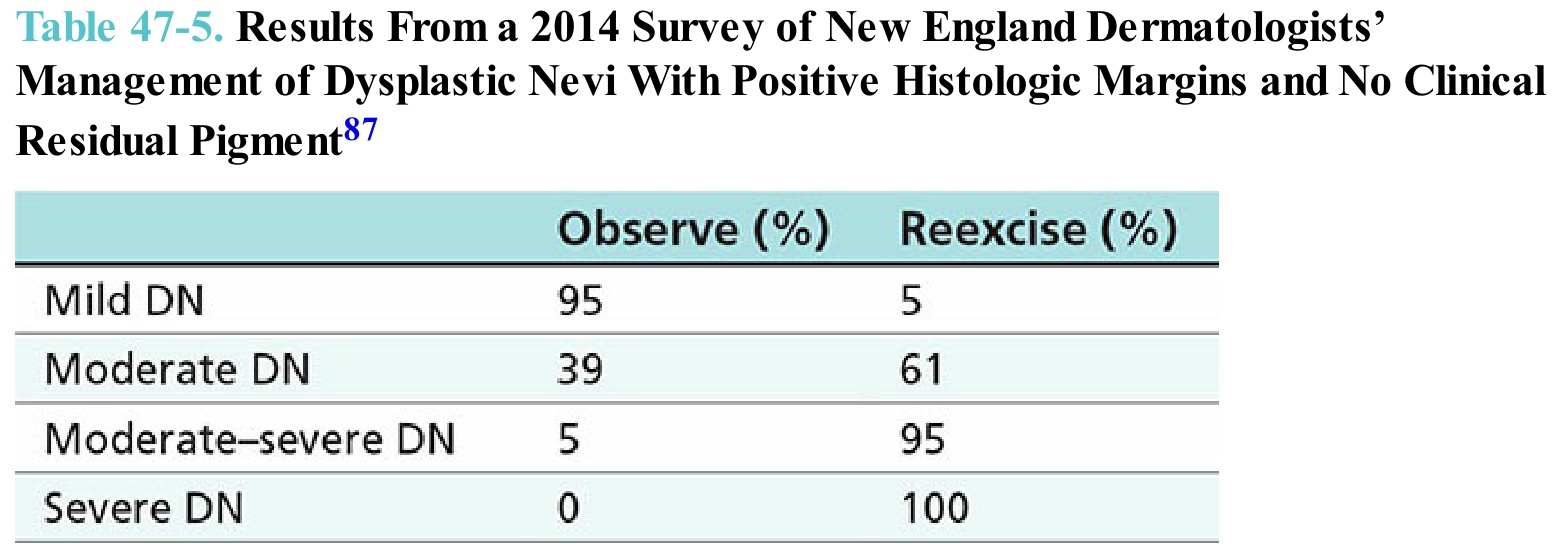
Table 47-5. Results From a 2014 Survey of New England Dermatologists’ Management of Dysplastic Nevi With Positive Histologic Margins and No Clinical Residual Pigment87