Fusiform excision
Fusiform excision
The fusiform or elliptical excision is a versatile technique that is a cornerstone of dermatologic surgery and the definitive removal of atypical pigmented lesions. The excision should ideally encompass at least a 2-mm margin of normal skin around a pigmented lesion, and the fusiform design results in a defect three to four times longer than the width of the planned excision (Fig. 47-4).82 The incision extends to the subcutis and should preferably be oriented such that the scar lies parallel to relaxed skin tension lesions. After surgical planning and orientation are established, the skin is marked with a surgical marker, cleaned and prepped in a sterile fashion. Local anesthesia is administered. Once the incision lines are made to the subcutis, a uniform thickness of tissue is removed through the subcutaneous fat in the fusiform shape. After appropriate undermining and hemostasis are achieved, closure can be achieved by several methods with the goals to provide precise wound approximation, maximal wound eversion, and reduce tension on the wound.83 A layered closure is generally performed. For a complete discussion of linear excision and repairs, see Chapter 18.
Fusiform excisional biopsies with 2- to 3-mm clinical margins are an ideal way to achieve an excisional biopsy of suspicious pigmented lesions, as both peripheral and deep margins can be accurately controlled by the clinician. As the goal of the excisional biopsy being to remove the complete skin lesion for accurate diagnosis, margins beyond 2 to 3 mm are not necessarily needed at the time of initial removal. If the suspicious pigmented lesion is believed to represent melanoma, the possibility of a follow-up wide local excision with sentinel lymph node biopsy must be considered, and the clinician should be mindful of the orientation and size of the initial excision. This is important to allow for the greatest chance of closure of a second, wider excision and accurate sentinel lymph node mapping. Reexcisions of DN are also typically performed in a fusiform fashion to ensure complete removal of any residuum, with some clinicians favoring a 5-mm reexcision of severe DN via a fusiform excision.
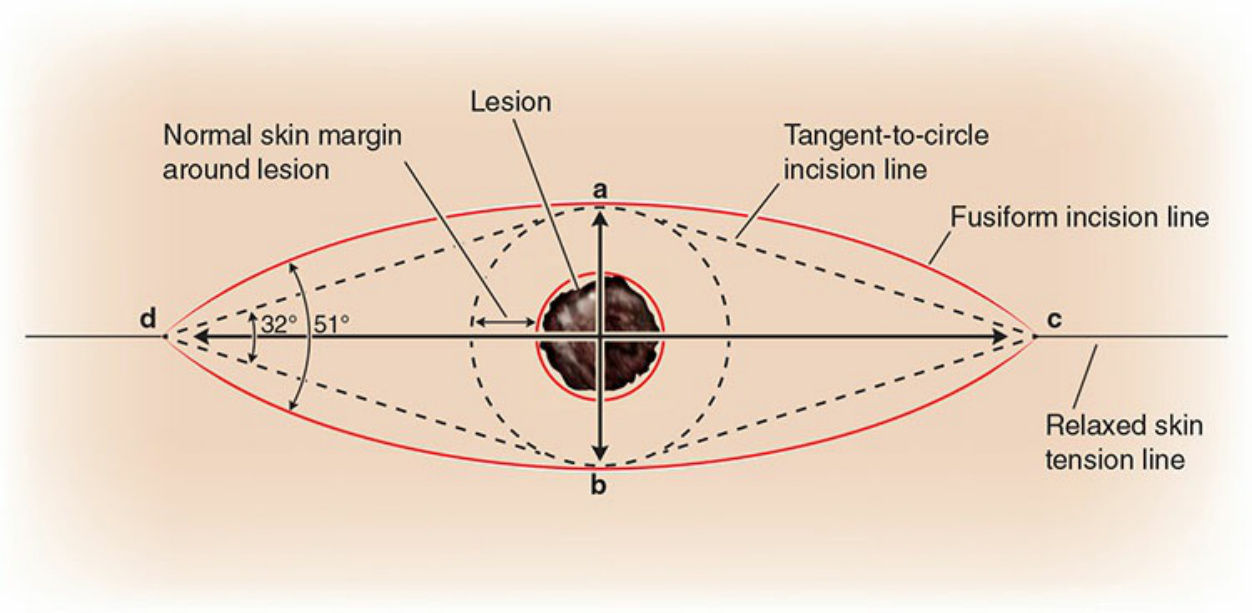
Figure 47-4. The fusiform excision.