Shave/saucerization biopsy and excision
Shave/saucerization biopsy and excision
Shave biopsies and excisions of pigmented lesions are rapid, commonly performed procedures that in certain clinical scenarios may result in comparable outcomes with punch biopsies or full-thickness skin excisions.77,78 In general, this procedure can be performed as a shave or saucerization using a sterile, flexible razor blade. Clinicians may choose to use either a 15-blade with a handle, a split sterile flexible razor blade, or a DermaBlade®. The skin is first anesthetized with an intradermal injection, which slightly elevates and tumesces the lesion and may make it easier to perform the biopsy. The nondominant hand is used to stabilize and hold the skin taut during the biopsy. Biopsies performed superficially may leave residual pigment either as a central dot or a peripheral rim.78 This can be prevented by increasing the downward angle of the razor
blade and lateral pressure. Another option for increasing the depth of the shave is to pinch the tissue beneath the nevus to create greater convexity of the area to be removed. Deeper shaves lead to more extensive wounds that may be associated with a depressed scar.79 A 15-blade with handle may be used for saucerization of suspicious pigmented lesions in areas of higher tension such as the midback. In the saucerization technique, a 1- to 2-mm margin of normal skin around the lesion can be marked and scored by applying light pressure to the blade along the marking. This allows for control over the peripheral margins of the biopsy. Light, continuous pressure is then applied tangentially through the dermis to the scored areas to release the skin specimen. The removed specimen is convex on its undersurface (Fig. 47-3).73,80
Larger shave excisions and saucerizations may take longer to heal than incisions repaired with sutures, and patients should be educated to continue wound care until the skin is healed completely. Patients who heal with hypertrophic scars or keloids may prefer punch or elliptical excisions. However, most patients consider the scars following shave biopsy to be acceptable and preferable to other methods such as more
invasive excisions into the deep dermis or superficial subcutaneous layer (Fig. 47- 3).73,80 The shave biopsy technique has been associated with a higher risk of recurrence of pigmented lesions.81 In general, shave biopsies are more superficial than punch or elliptical excisions and are more likely to leave a positive deep margin, though clinician experience with the technique likely plays a role in how accurately a pigmented lesion is removed, and many pigmented lesions are effectively biopsied in this manner.
Although excisional biopsies of suspicious pigmented lesions are favored, certain scenarios may cause a clinician to favor a shave incisional biopsy of a pigmented lesion. These scenarios include larger diameter lesions difficult to remove in total; lesions in certain anatomic areas (acral and face); and lesions removed that are of lower clinical suspicion, such as those removed for irritation or cosmesis (Table 47-4). Limitations, such as sampling error and inability to assess deeper tissue should be considered with shave incisional biopsies. As with any partial incisional biopsy, any clinical pigmented lesion remaining after the biopsy should be monitored for the possibility of melanoma.
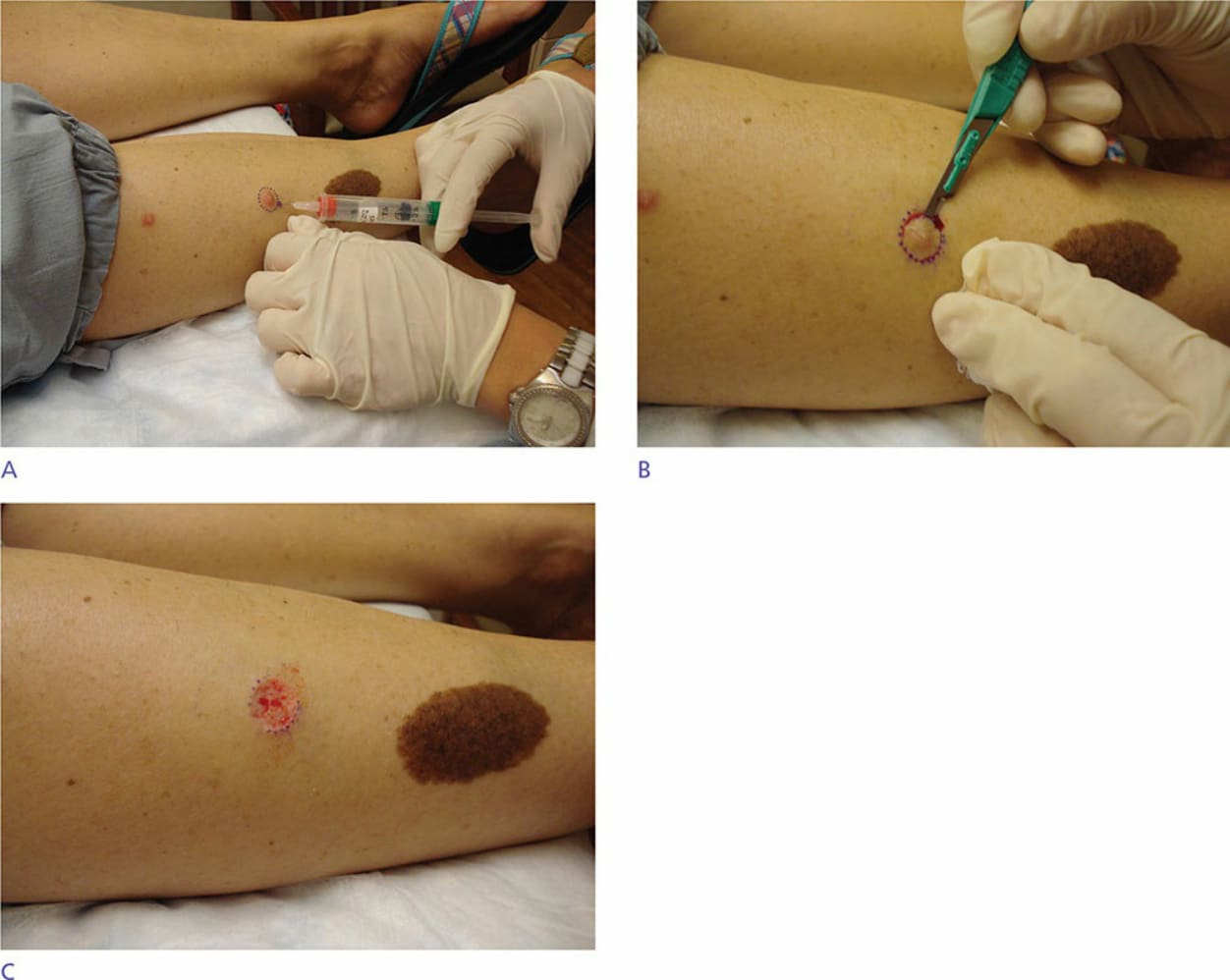
Figure 47-3. (A) Saucerization excisional biopsy technique: Lesion is marked with a surgical pen with 2- to 3-mm clinical margin of surrounding normal skin, cleaned, and anesthetized. (B) Marked lesion is scored around the margin, then blade is tangentially and continuously drawn through the dermis to scored areas. (C) Appearance of wound after removal of lesion.
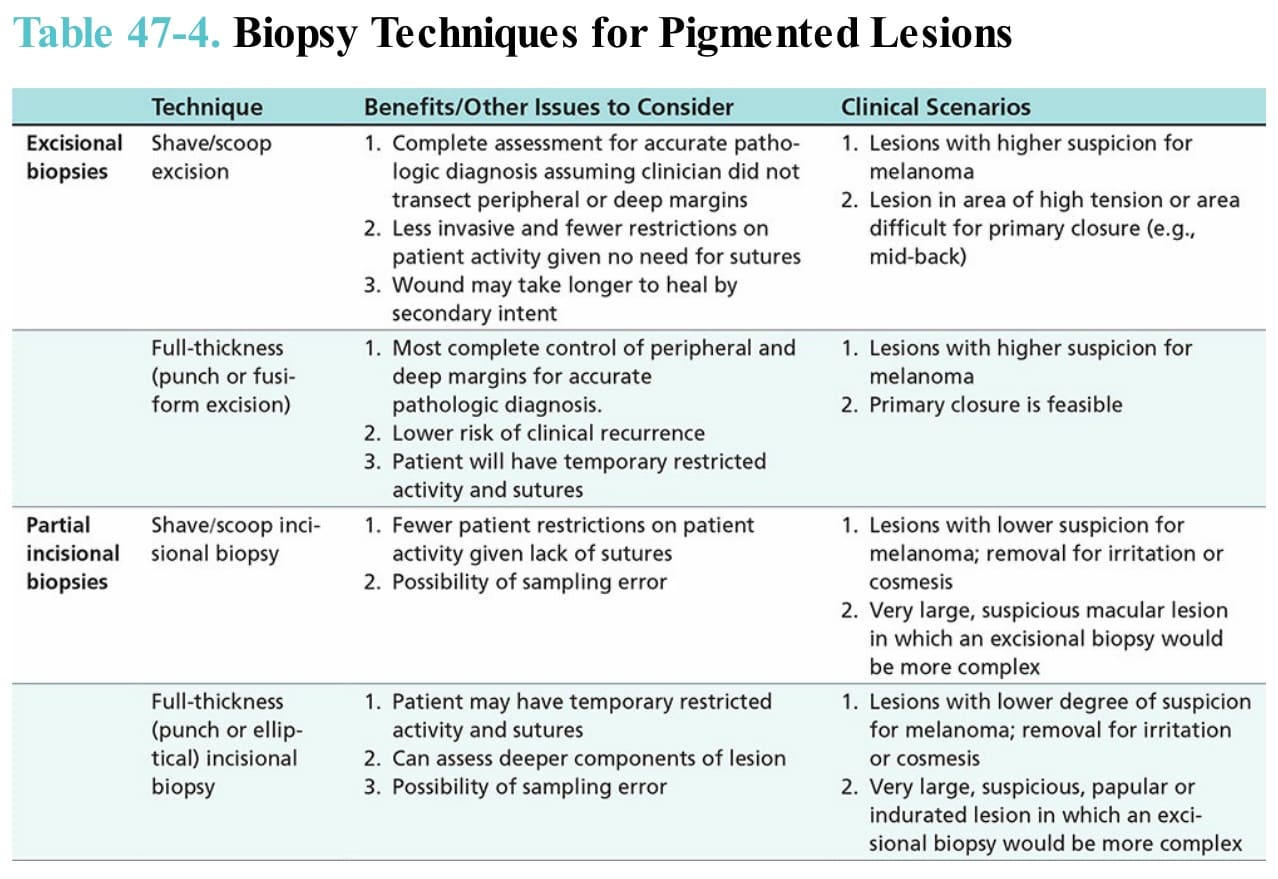
Table 47-4. Biopsy Techniques for Pigmented Lesions