Punch biopsy/excision
Punch biopsy/excision
Prior to performing a biopsy, the sites are typically cleaned with 70% isopropyl alcohol, anesthetized using lidocaine with epinephrine.73 A punch biopsy relies on a metal cylinder with a sharp circular cutting edge to remove a full-thickness sample of skin, usually ranging in diameter from 2 to 8 mm. For pigmented lesions, the punch diameter should ideally extend at least 1 mm beyond the clinical pigment, with the goal of complete removal of the lesion. The clinician can score the skin around the pigmented lesion with light pressure to assess the correct-sized punch and map the best location for the punch to create clear clinical margins. The punch instrument is then rotated in a circular motion between the fingers until the instrument cuts through the dermis, meeting less resistance in the subcutaneous fat (Fig. 47-2), at which time forceps are used to elevate the section and cut it away from the subcutaneous tissue.73
subcutaneous fat is felt. (C) The atypical pigmented lesion with surrounding 2 mm of normal skin is released by the punch technique, and the clinician cuts at the base of the tissue before placing sutures.
Hemostasis is achieved usually with one to three interrupted sutures; adhesive tape or a buried dermal suture can also be used for larger defects.74 Nonabsorbable sutures are removed, in general, between 5 to 14 days postprocedure depending on anatomic site. Alternatively, if the punch is very small or the wound is very difficult to close primarily due to tension or other considerations, it may be appropriate to allow the wound to heal by secondary intention, in which case hemostasis can be achieved using gelfoam if desired. Electrocautery, aluminum chloride, or other hemostatic agents are less desirable because these methods may impact wound healing.75 Punch biopsy sites that heal by secondary intention may be appropriate for younger patients who can easily care for their biopsy site, and may have outcomes comparable with 4-mm punch biopsies on the trunk or extremities that are closed with sutures. Older patients and those requiring larger punch biopsies may not be good candidates for healing through secondary intention because the outcomes are suboptimal in terms of postoperative pain, healing time, and scar formation. Adhesives are insufficient for closing punch biopsies because they do not bear adequate tension.76An incisional punch biopsy by definition samples a portion of a larger lesion. For pigmented lesions, this may be considered in specific scenarios (Table 47-4). In general, although excisional biopsies are the preferred method of removal of lesions suspicious for melanoma, some pigmented lesions may be more difficult to remove in total due to size or sensitive anatomic area (such as on the face or feet), and clinicians may choose to sample a portion of these first. While not allowing a complete lateral architectural assessment of a lesion, the full depth of a lesion could be accurately assessed by punch biopsy, and therefore is desirable for palpable or indurated suspicious lesions.
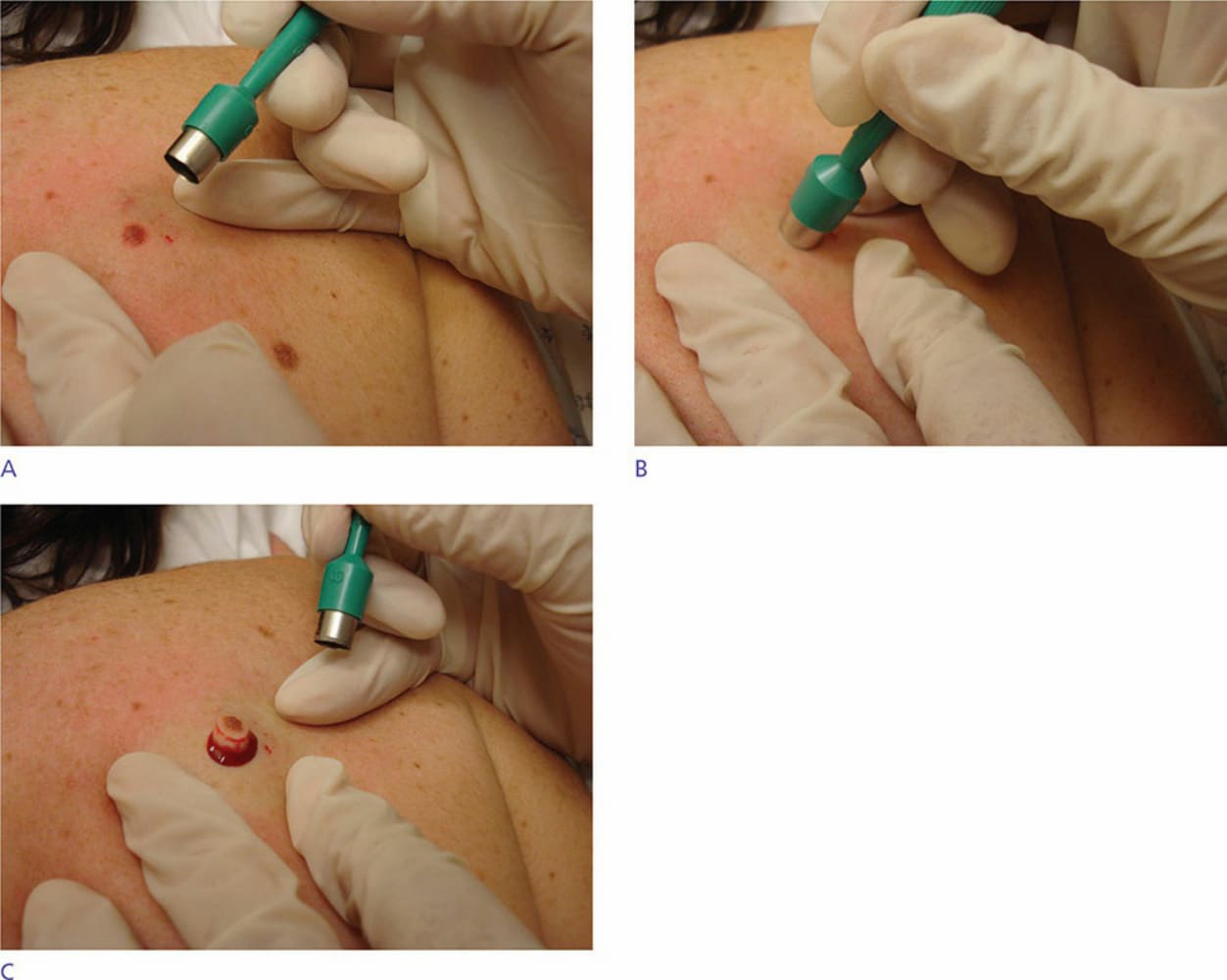
Figure 47-2. (A) Punch excisional biopsy technique (8-mm punch): Skin is held taut by hands and punch location is approximated to allow for margin of normal skin surrounding lesion. (B) Punch device is placed around lesion and rotated between fingers while applying pressure downward through the dermis until less resistance of the
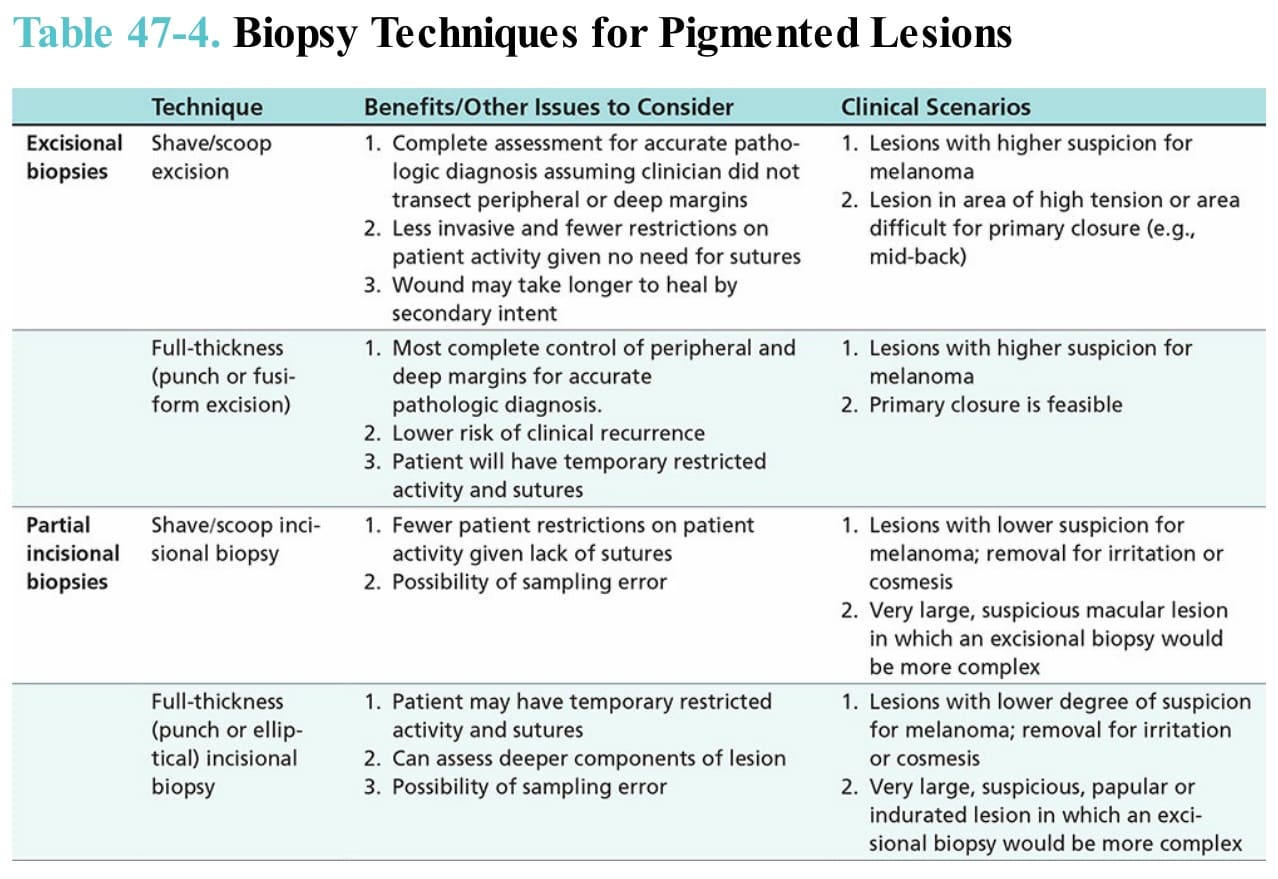
Table 47-4. Biopsy Techniques for Pigmented Lesions