Sentinel lymph node biopsy technique
Sentinel lymph node biopsy technique
Intraoperative node mapping is performed using a combination of vital blue dyes and radiopharmaceuticals with gamma probe detection. The most commonly used dyes are methylene blue and isosulfan blue, which are independently associated with a sentinel node detection rate of 82% to 95%.42,43 Comparison studies have shown no difference between dyes.44,45 Isosulfan blue costs more, is associated with urticaria or rash in 1% to 3% of patients, and has a 0.1% to 0.5% risk of anaphylactic reaction.46 Methylene blue has a rare association with local skin necrosis following intradermal injection.47 Dye is injected intradermally around the lesion or biopsy site. The rate of lymphatic migration to sentinel node is variable, requiring approximately 15 to 30 minutes in most cases, and depends on the location and distance from the nodal basin (e.g., extremity vs. trunk, distal vs. proximal extremity). Soft-tissue lymphatics are concentrated in the dermis, and therefore intradermal injection theoretically provides optimal uptake. In general, the dye is injected in the operating room prior to incision, which provides sufficient time for nodal uptake.
Combined use of blue dye and radioisotope lymphoscintigraphy, typically technetium 99 (99mTc), improves the sentinel node detection rate from 98% to 99%.48,49 Radioisotope lymphoscintigraphy was pioneered in the 1970s, though application of intraoperative gamma probe detection appeared in the 1990s (Fig. 46-7).50 99mTc bound to colloid was found to be an effective agent due to its increased photon flux and absence of beta radiation. Multiple colloid agents with variable sizes and lymphatic passage rates have been studied, including albumin and sulfur colloid.51 Antimony sulfide is another effective compound for lymphatic mapping, but is not available in the United States. More recently, new techniques for radiolabeled molecular targeting of nodal tissue have been studied in a clinical trial setting; these agents may provide faster ejection site clearance, allowing for shorter lag time between injection and surgery, and potentially more accurate sentinel node radiolabeling.52 Radioisotopes are larger than dyes, and therefore require several hours to concentrate in the nodal basin. Therefore, patients are required to either undergo injection the night before surgery, or arrive several hours early on the same day.51 Uren et al. evaluated lymphatic flow rates in 198 patients with melanoma using 99mTc, and found mean flow (cm/min) to be lowest in the head or neck (1.5) and highest in the distal leg and foot (10.2). Rates were also higher for patients with residual inflammatory reaction after excisional biopsy.53 As with dye, intradermal injection appears to be more effective than subcutaneous infiltration.54
Importantly, 99mTc will remain concentrated in the sentinel node for up to 24 hours after injection, although its half-life for gamma emission is only 6 hours.
Whereas upper and lower extremity melanomas reliably drain to the ipsilateral axillary and groin nodal basins, respectively, trunk melanomas more frequently drain to multiple or contralateral basins, which makes node staging and treatment challenging in these patients.55,56 Gordon et al. evaluated 859 patients with cutaneous melanoma, 465 located on the trunk and 394 on the extremities. Trunk melanomas were found to have significantly greater rates of multiple (31% vs. 7%) and contralateral sentinel nodes (25% vs. 1%). There was no difference in uncommon nodal occurrence between groups (7% vs. 8%), defined as nodes not located in the groin or axilla. Trunk melanomas were associated with significantly worse prognosis, consistent with multiple prior study findings.55 Similarly, SLNB for head and neck melanoma (HNM) is technically more challenging, in part due to the presence of over 300 nodes in a confined area, and melanomas in this region often drain to multiple, contralateral and uncommon sites. In a review of over 3,400 HNMs, the sensitivity of SLNB by standard technique was 80% to 100%, with a false-negative rate up to 20%.57,58 Single-photon emission computed tomography (SPECT) and CT may provide added value regarding detection of sentinel nodes for HNMs.59 Ultimately, SLNB is a complex procedure dependent on multiple factors. Some patients will have unexpected or irretrievable nodes. Effective technique relies on the competence of and communication among nuclear medicine specialists, the surgeon, and the pathologist.
Morton et al. provided the first technical description of SLNB using 0.5 to 1 mL of vital blue or isosulfan dye injected intradermally around the lesion or biopsy site.33 Although the principles have largely remained the same, the advent of radiocolloid has
allowed for transcutaneous localization resulting in smaller incisions placed directly over a hot signal. Variables including tracer type, volume, injection site, waiting period, and surgeon experience have been extensively studied.
The procedure is performed as follows: Radiation technologists perform intradermal injection of 99mTc preoperatively, typically in sites immediately surrounding the biopsy scar, with an appropriate lag time for lymphatic migration to sentinel nodes. For operations that take place early in the morning, it may be necessary to inject the isotope in the evening prior to surgery. After anesthesia induction in the operating room, and prior to prepping and draping, the basins of interest are tested with the gamma probe for a hot signal. The point of maximal signal is marked for an incision. Next, blue dye is injected intradermally, and the tissue massaged. Both the site of WLE and SLNB are prepped in the same sterile field.
Prior to making an incision for the sentinel node biopsy, the gamma probe is again used to confirm the location of maximal signal. Patients undergoing axillary node biopsy or dissection should be asked about joint mobility or instability issues preoperatively. Local anesthetic is injected into the dermis to provide postoperative pain relief. The incision is ideally made along relaxed skin tension lines. Electrocautery or sharp dissection is used to dissect into the subcutaneous tissue, coagulating small vessels to ensure hemostasis. Once in the subcutaneous layer, dissection continues toward the node basin (Fig. 46-8). Constant testing of the surgical bed with the gamma probe helps focus the dissection in the appropriate direction of the sentinel node, limiting unnecessary tissue damage and lymphatic disruption. Mapping the migration of blue dye supplements this process. The advantages of a small incision include a better cosmetic result, reduced pain, and decreased risk of wound complication. However, this must be balanced against the difficulty of dissecting into a deep, fatty cavity, particularly within the axilla. Richardson retractors held by the assistant may help with exposure, and use of tonsil clamps to grasp the deep, fatty tissue provides improved visualization of the surgical bed. Metal clips may be applied to transected tissue that appears to contain lymphatics or blood vessels to prevent lymphocele and postoperative bleeding.
Each node typically has a vascular pedicle that bleeds with transection, which should be identified and clipped or cauterized as the plane along the capsule of the node is freed from the surrounding tissues. Care must be taken not to transect nodes in order to avoid potential oncologic compromise.
After the node is removed, node radioactivity is quantified with the gamma probe. The surgical bed is re-evaluated for hemostasis, and the probe is then re-inserted for identification of any remaining radioactive nodes. Nodes that have signal in greater than 10% of the sentinel node should be removed. It is important to note that if the tip of the probe is directed toward the primary lesion, a false-positive signal will occur from the very large amount of radiocolloid at the injection site. If the location of the primary tumor is anticipated to create this problem of “shine through,” the primary tumor should be excised as the first part of the procedure to eliminate the source of the radioactivity.
Ideal circumstances would permit accurate intraoperative histopathologic node analysis, preventing a second surgery for patients with positive nodal disease that require lymphadenectomy. However, the sensitivity of intraoperative imprint cytology and frozen section results remain relatively low for melanoma, in the range of 50% to 75%.60 Given this finding, coupled with the low baseline prevalence of nodal metastases, routine intraoperative analysis is not typically recommended.61
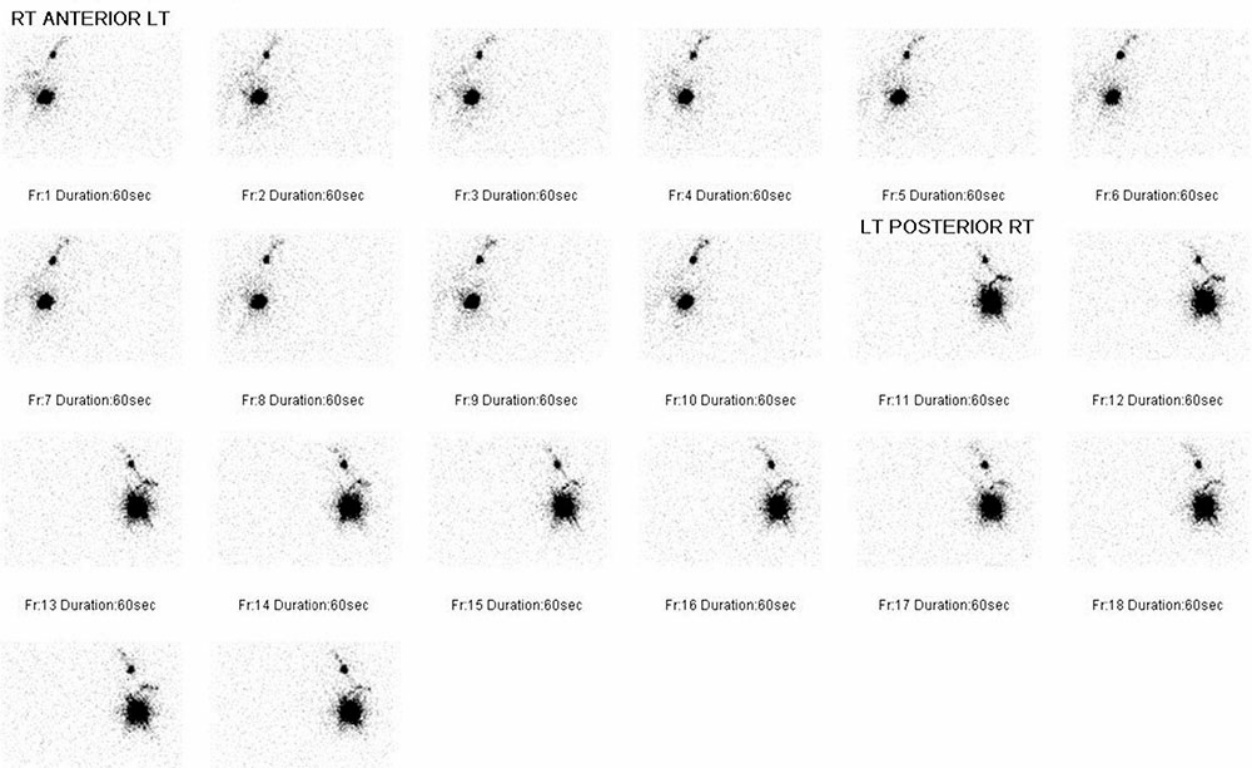
Figure 46-7. Lymphoscintigram.
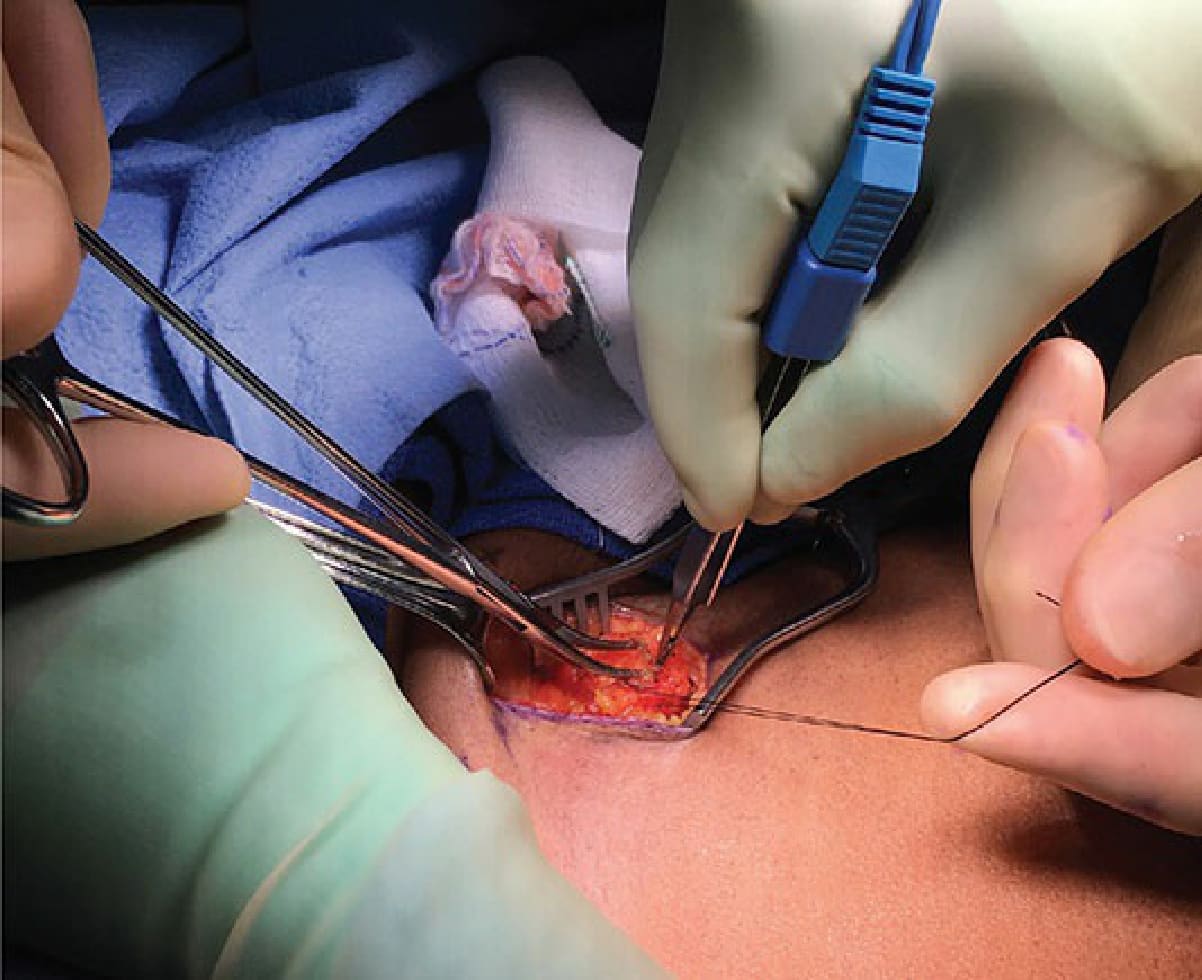
Figure 46-8. Dissection of sentinel lymph node for biopsy.