Cutaneous biopsy techniques for melanoma
Cutaneous biopsy techniques for melanoma
For undiagnosed patients presenting with an abnormal pigmented skin lesion, multiple biopsy techniques are available. Breslow depth is the most important histopathologic prognostic determinant in melanoma, and is used to guide excision margin width and indication for SLNB.5 Choice in biopsy technique is influenced by several factors including physician specialty, resources, and efficiency. Excisional biopsy with 2-mm margins is ideal for highly clinically suspicious pigmented lesions, though it is more time-consuming than shave biopsy, and a deep (scoop) shave biopsy is usually adequate for most lesions.6 Bolshinsky et al. evaluated their experience of 807 WLE specimens
after diagnosis with complete excisional biopsy, and found residual disease in 4.2% of cases, with predominance of lentigo melanoma subtypes.7 WLE is not recommended for initial treatment due to the low incidence of melanoma diagnosis among all pigmented lesions, as well as potential impact on sentinel node mapping. There is no role for frozen sectioning in melanoma biopsy.
Particularly with melanoma, partial biopsy techniques including shave and punch are subject to error, though debate continues whether the degree of error is within an acceptable range.8 Inaccurate biopsy sampling may result in incorrect staging, inadequate subsequent wide resection margin, and missed indication for SLNB. Several studies have evaluated partial biopsy in cutaneous melanoma, and found that it has no influence on prognosis. Molenkamp et al. reviewed their experience with 471 melanoma patients, and concluded that neither the biopsy method nor the presence of cells at the deep margin during excision had a detrimental effect on survival.9 More recently, Mills et al. evaluated 709 melanoma patients, of which 23% underwent punch biopsy and 34% underwent shave biopsy. Partial biopsy techniques resulted in more positive margins at WLE, but had no impact on disease-specific survival.10 Similarly, Mir et al. reviewed their experience of 479 patients, and found significantly higher primary lesion transection rates with partial biopsy techniques, though no effect on overall survival.11 Egnatios et al. reviewed 609 melanoma patients, 70% underwent shave or punch biopsy, 39% had positive margins after biopsy, and 10% had tumor upstaging after WLE, though none of these factors influenced overall survival on multivariate analysis.12 In addition, there is no evidence that partial biopsy may result in increased sentinel lymph node (SLN) micrometastases or locoregional and distant recurrences.13
With shave biopsy, there is risk of potentially transecting the base of the lesion, and approximately 20% of lesions will have a positive deep margin at the time of surgery.6 Kaiser et al. reviewed 853 patients with cutaneous melanoma that underwent shave biopsy, and found that this technique underestimated the depth of lesions by over a millimeter in 12.5% of patients, of which 4.7% required further surgery after initial WLE.14 In a separate review of 600 patients by Zager et al., the margin of error was lower; only 3% of lesions were upstaged at WLE, 2% required additional WLE, and 1% required SLNB.8 Mir et al. reviewed 240 cases, of which 128 underwent shave biopsy. Of these, 22% had positive deep margins, a significantly greater proportion than with punch or excisional techniques.11 This was corroborated in a review of 240 cases by Stell et al., who similarly had a deep positive margin rate of 22% with shave biopsy.6 For this reason, most dermatologists who perform shave biopsies for melanoma tend to take a deep and broad sample (scoop shave), and this tendency likely explains the broad variation in positive deep margins between studies. The American
Academy of Dermatology consensus statement suggests an excisional biopsy, but includes a deep scoop shave as an excisional technique. Therefore, if a shave biopsy is performed, it should be of ample breadth and depth to capture the full extent of the tumor.
Punch biopsy can be a useful technique under appropriate circumstances, and though this approach often leaves a positive peripheral margin, it is effective for measuring the depth of invasion. Biopsy should be taken from the most raised or pigmented area, which presumably corresponds to the deepest portion of the lesion, though this is subject to error. If there is significant clinical heterogeneity to the lesion, multiple punch samples may be taken, with emphasis on evolving regions. Hieken et al. reviewed their experience with 332 cutaneous melanoma patients, and found that T-stage changed in 8% of patients, of which 59% underwent punch biopsy, and treatment recommendations changed in 18% of punch biopsy patients.15 Ng et al. reviewed 2,470 melanoma biopsies, including excisional, shave and punch specimens. They found a 3.4% rate of false-negative misdiagnoses, the majority stemming from partial biopsy techniques (punch OR 16.6, p < 0.001; shave OR 2.6, p = 0.02; relative to excisional). Partial biopsy was associated with increased microstaging error as well (punch 34%, OR 5.1, p < 0.001; shave 19%, OR 2.3, p < 0.001; relative to excisional). Misdiagnosis and inaccurate microstaging resulted in 37 (1.5%) adverse outcomes, all related to the persistence or progression of primary disease. General practitioners were six times more likely than dermatologists to misdiagnose with partial biopsy techniques. Acral lentiginous, desmoplastic, and nevoid melanomas were most commonly subject to inaccurate diagnosis and staging.16 The high probability of positive peripheral margins and an approximately 10% to 20% chance of tumor upstaging on final pathology should be considered when approaching wide excision for patients after punch biopsy. A summary of biopsy techniques in melanoma is listed in Table 46-2.
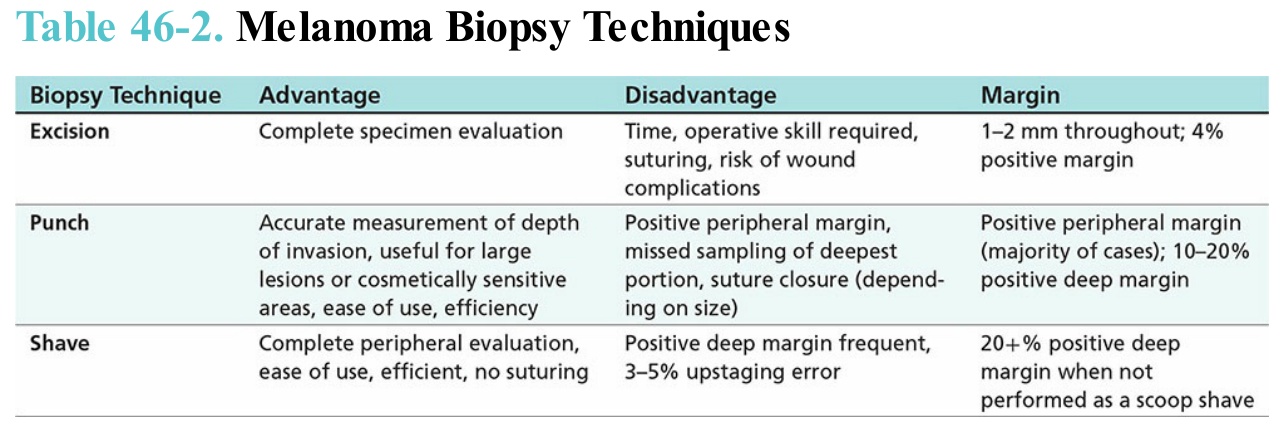
Table 46-2. Melanoma Biopsy Techniques