PREOPERATIVE EVALUATION
PREOPERATIVE EVALUATION
Preoperative evaluation begins with clinical history and physical examination. In most cases, a diagnosis will have been established prior to surgeon evaluation. The patient should be screened for symptoms of metastatic disease (constitutional, lymphatic, hepatic, pulmonary, gastrointestinal, skin, musculoskeletal, neurologic review of systems). Physical examination includes inspection of the primary lesion, as well as thorough examination of the entire skin, including the hairy scalp, and oral and genital mucosa to assess for satellite or synchronous lesions. Careful palpation of all nodal basins should be performed, as well as palpation for in-transit metastases. For asymptomatic patients diagnosed with primary melanoma without clinical evidence of nodal spread, there is no evidence to support routine laboratory or imaging investigations for metastatic disease. These tests have high false-positive rates,
resulting in more unnecessary testing and anxiety. A focused investigation for distant disease should only be pursued based on objective signs or symptoms.3
Clinically palpable nodal metastases will be present at the time of diagnosis in a small percentage of patients. Nodal spread should be histologically confirmed, preferably with fine needle aspiration (FNA), which can be done either by palpation or with ultrasound (US) guidance in the outpatient setting. Other biopsy methods include core, incisional, and excisional techniques, which are more invasive and rarely necessary. In some cases, palpable nodes represent reactive lymphadenopathy resulting from local inflammation at the primary biopsy site. Nodal basin US may be considered for equivocal nodal examination findings, though there is no evidence for the use of screening US as a replacement for sentinel lymph node biopsy (SLNB) in clinically node-negative patients.4 A complete staging workup is required after confirmation of nodal metastases. This includes magnetic resonance imaging (MRI) of the brain, and imaging of the chest, abdomen, and pelvis with computed tomography (CT), positronemission tomography (PET), or both. For melanoma of the extremities and head and neck, axial CT imaging of the affected nodal basin is helpful to determine disease burden for operative planning.3 A summary of recommended components for preoperative clinical evaluation is shown in Table 46-1.
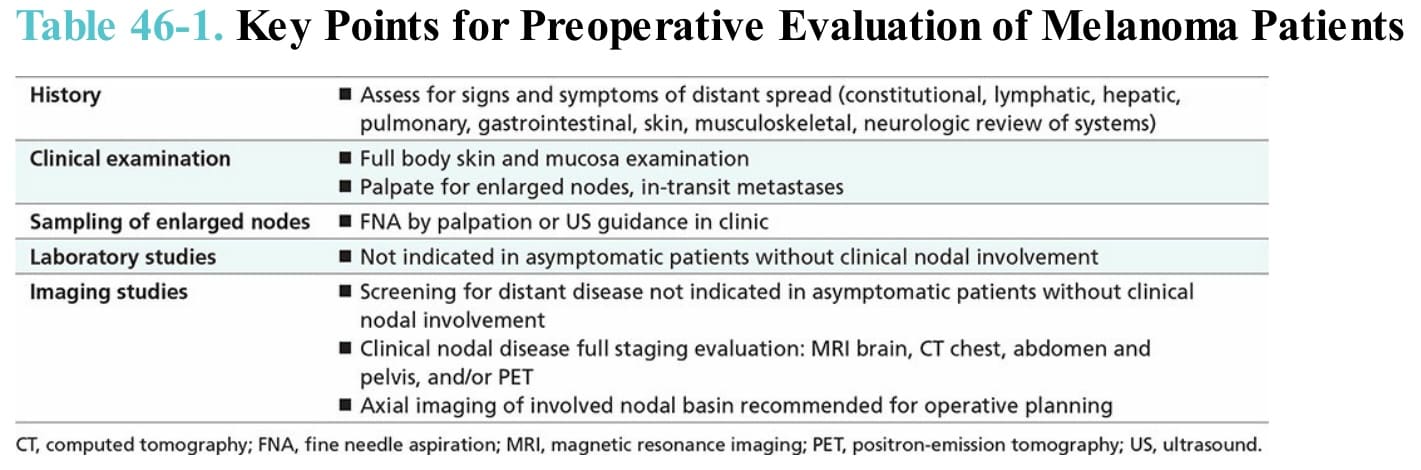
Table 46-1. Key Points for Preoperative Evaluation of Melanoma Patients