Fascial Flaps
Fascial Flaps
Wounds that are devoid of periosteum and are too large to close primarily with a flap benefit from being resurfaced, at least in part, with a vascular covering. As previously discussed, chiseling the outer table of the bone can induce granulation, though reports of air emboli associated with this technique are of concern and serve as a motive to seek alternative approaches. Options frequently employed by dermatologic surgeons include hinge flaps (Fig. 44-17) and fascial transposition flaps (Fig. 44-18). The movement of adjacent fascia over the wound to cover, at least in part, the denuded bone provides a vascular source for granulation tissue and ultimately permits grafting, which is usually delayed as the vascularity of a newly placed fascial flap may not be sufficient to support the graft.
The fascial transposition flap is essentially a banner flap where a rectangular flap is raised upon a vascularized base, elevated, and then transposed onto the wound base (Fig. 44-19). This flap may be harvested through incision and mobilization from the subgaleal approach; however it is generally easier to create access to the fascia by making an incision of the skin overlying the flap approximately perpendicular to the wound. The reflection of the skin from either side of this incision exposes the underlying fascia. By doing so, the fascia can be directly accessed, incised, and mobilized. The fascia is not very flexible or elastic, and the dimensions of the flap must accommodate these limitations. The wider the flap base, the more limited will be its mobility. A long and narrow flap is therefore preferred, in part due to the diminishing reach and pivotal restraint of the flap as it is transposed into the defect. The flap is then sutured into place with absorbable sutures and standard occlusive bandaging is performed and left in place for up to a week. Granulation tissue will begin forming over the flap shortly and ultimately provide a satisfactory vascular base suitable for delayed grafting or second intention wound healing.
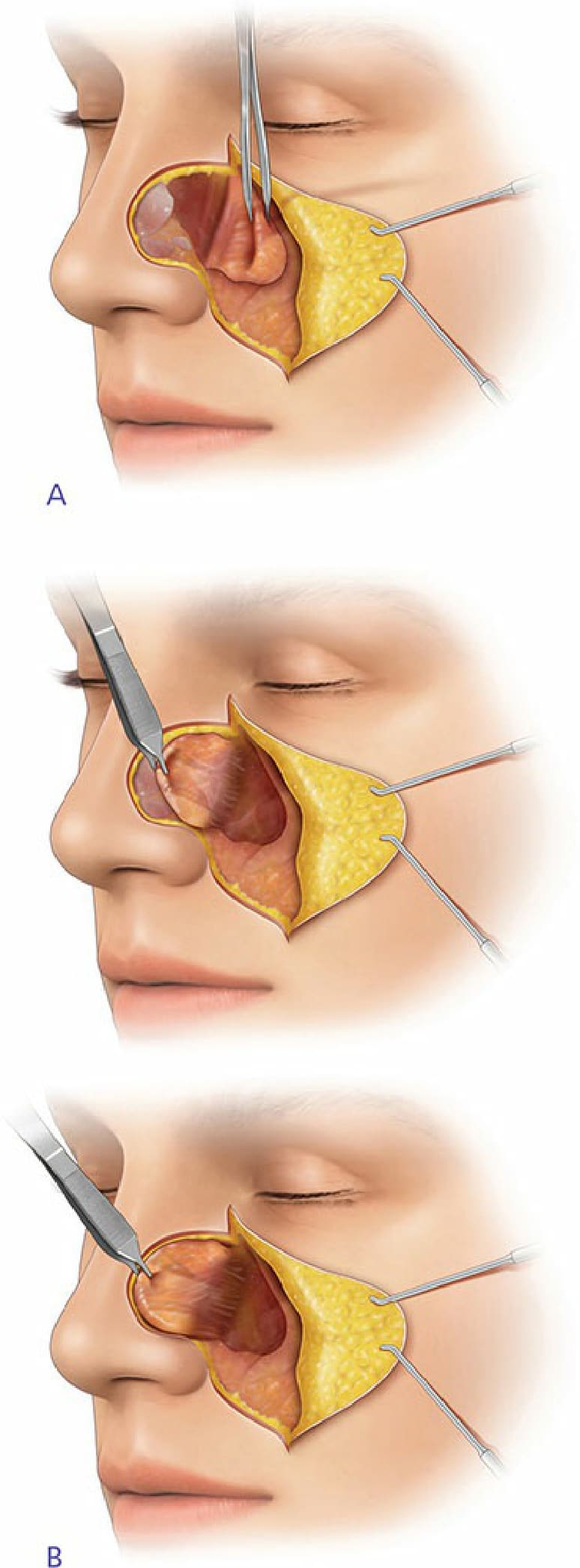
Figure 44-17. The hinge flap.
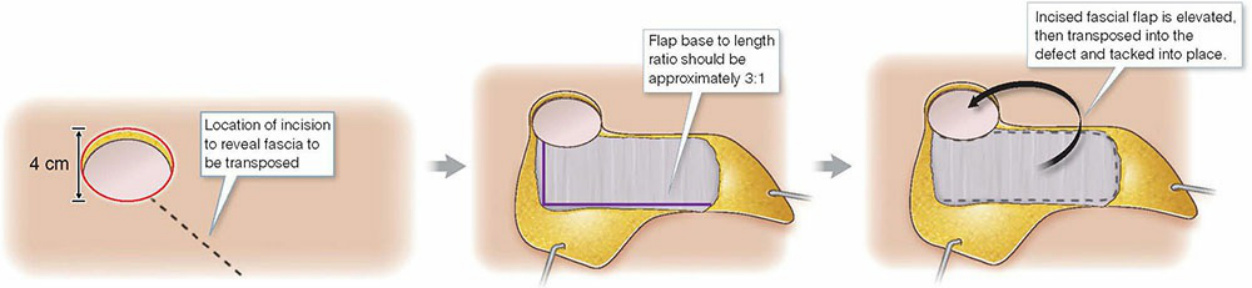
Figure 44-18. The fascial transposition flap.
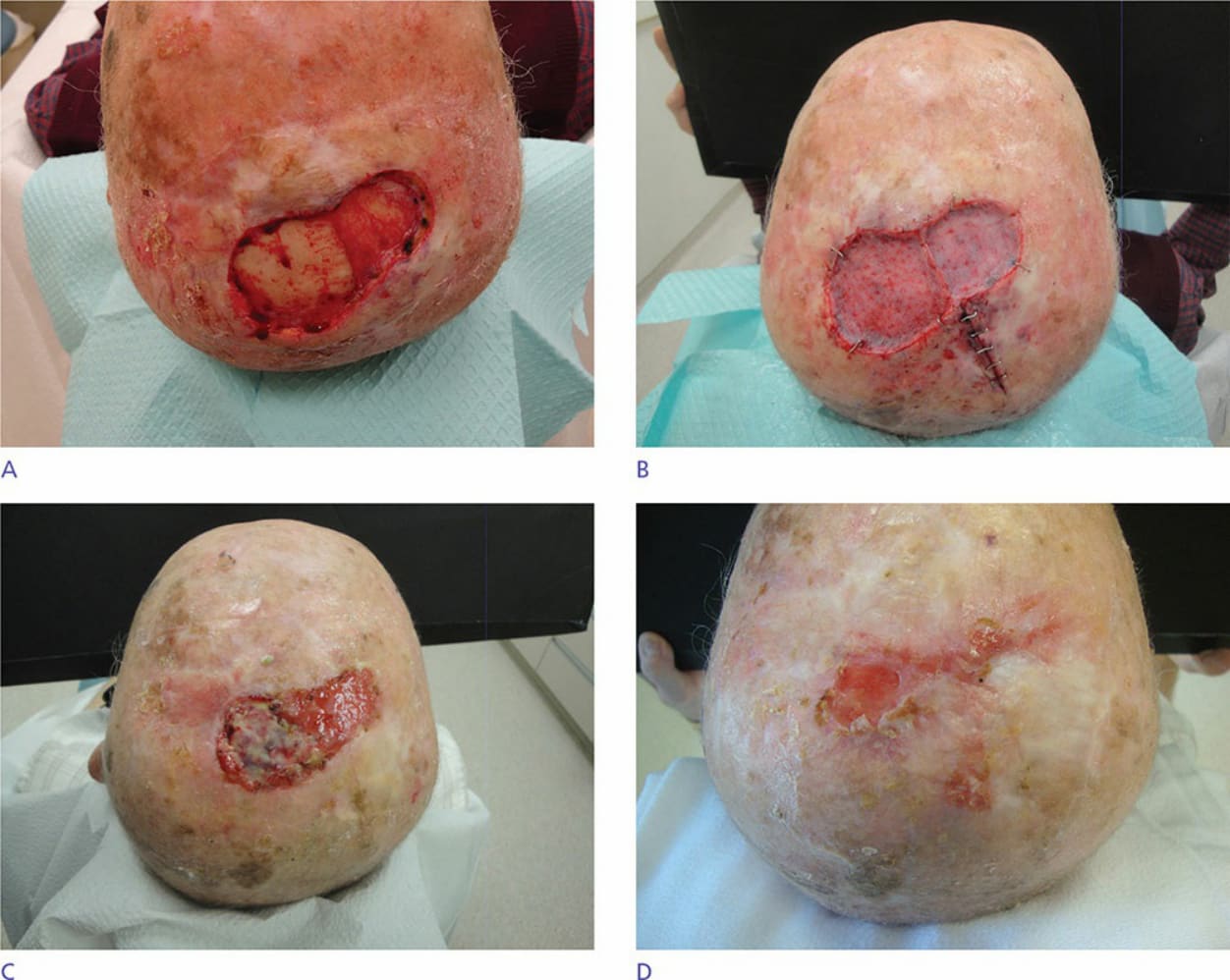
Figure 44-19. (A) Defect after Mohs excision of invasive squamous cell carcinoma. Defect extends to and includes periosteum for the left half of the defect. (B) Postoperative view after fascial transposition flap. Incisions perpendicular to the wound and reflection of the skin facilitated access to the fascial flap which is based at the left posterior portion of the wound. The flap and the right portion of the defect which did not extend through periosteum are covered with xenograft. (C) One-month postoperative healing by second intention. (D) Four months postoperatively.