Flaps
Flaps
The skin of the scalp is largely inelastic, particularly on the crown, though laterally, skin overlying muscles (superior frontalis, temporalis, and occipitalis) may be more flexible.6 Thus, there are two imperatives when considering a flap repair on the scalp. First, the surgeon must be able to estimate the intrinsic elasticity of the scalp in order to plan the successful execution of the flap. Second, the surgeon must understand the mechanisms of tissue movement for each flap type. For instance, advancement flaps and rotation flaps are largely dependent on intrinsic tissue elasticity, while V-Y (island pedicle) flaps are dependent on the flexibility of the underlying tissue that comprises the pedicle. In contrast, transposition flaps are less dependent on intrinsic elasticity, but are very dependent on the laxity of the donor site (Fig. 44-15).7 Although interpolation flaps have been described in hair restoration, they are rarely used for reconstruction. Free flaps are useful and frequently employed for reconstruction of large defects on the scalp, but are beyond the scope of this chapter.
Scalp reconstruction with flaps may permit hair-bearing skin to be transferred from the donor site to a previously hair-bearing defect (Fig. 44-16). The thick, inflexible, and
inelastic characteristics associated with scalp skin make execution of flaps more challenging in this anatomic location, as flaps, by their nature, require a nearby donor site characterized by redundancy or laxity that can accommodate a loss of tissue.8
Therefore, scalp flaps may of necessity be larger or more involved (combining multiple flap types) than those performed in other areas.9 In planning the flap, an additional detail that must be considered in hair-bearing skin is the quantity and growth direction of hair within the flap and what its orientation will be once the flap is completed. For instance, when a defect is located on the lateral pate of a balding scalp and is adjacent to temporal or occipital scalp, the temporal or occipital skin may serve as an ample donor site. However, transfer of hair-bearing skin onto the bald scalp from a hair-bearing donor site may result in a highly conspicuous reconstruction. Furthermore, the orientation of the hair shafts may be incongruous with the surrounding hair adjacent to the wound.
Galea is sometimes incorporated within the flap, though including the inelastic galea may tether the flap and restrict movement more than if it was not included. Still incorporating the galea provides a robust substrate into which sutures can be placed.
Occasionally, flap closures on the scalp are used to displace a defect to a more convenient or less aesthetically conspicuous location, leaving the nascent donor site open. The donor site can then be allowed to heal by second intention using standard occlusive wound care, or be closed with a skin graft. This option is particularly useful when there is a dominant aesthetic need such as a defect toward the front of the scalp that can be displaced posteriorly or laterally to a more inconspicuous location.8
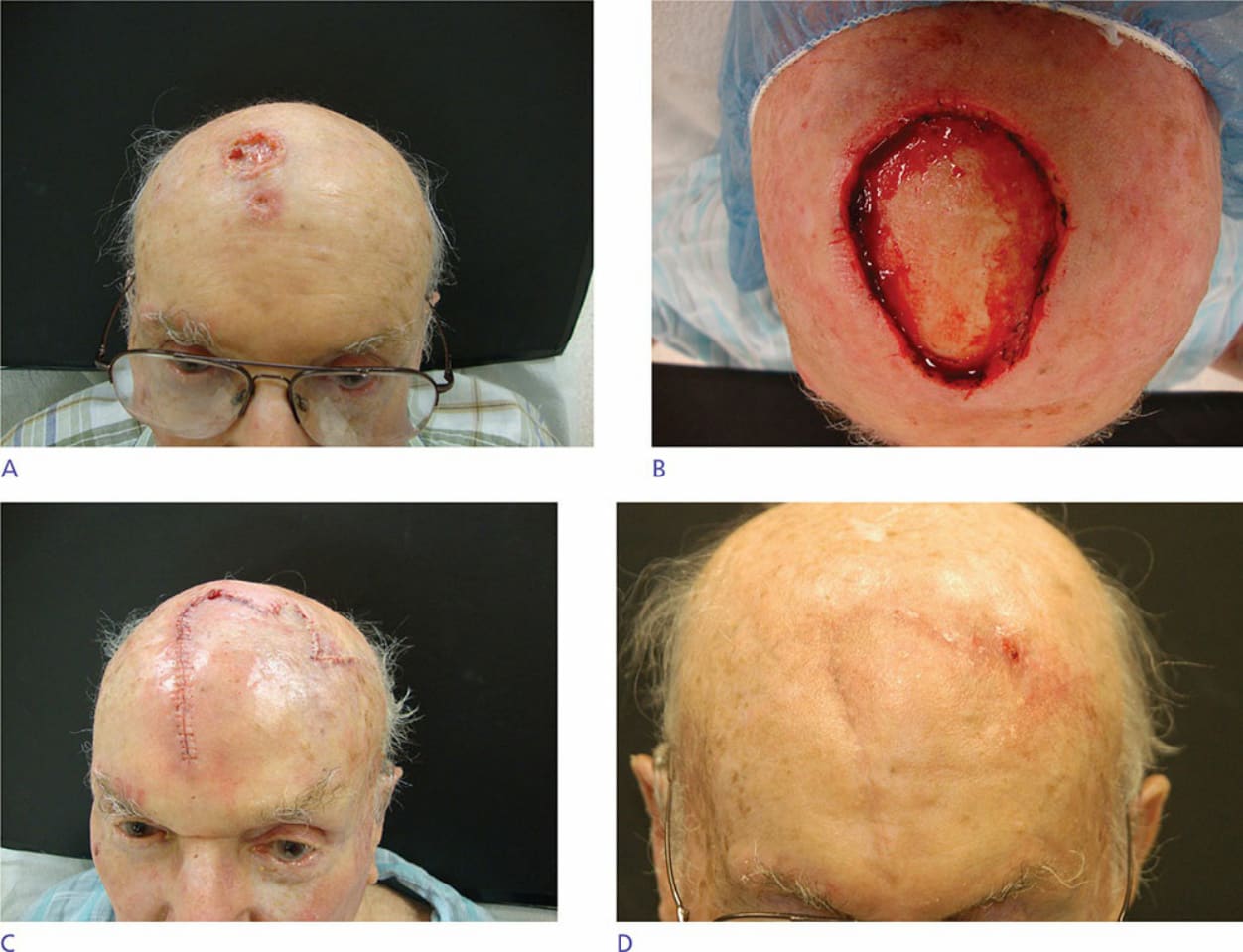
Figure 44-15. (A) Large squamous cell carcinoma preoperatively. (B) After Mohs surgery. (C) Large bilobed flap sutured into place. (D) One month postoperatively.

Figure 44-16. (A) Large Mohs defect on the vertex of the scalp. (B,C) Closure with rotation flap.