Pinch Grafts
Pinch Grafts
Pinch grafting is a simple variant of grafting that results in a hybrid graft with characteristics of both STSGs and FTSGs.3,4 The technique is simple but effective for certain clinical scenarios. Though this is not usually a first-line approach, it is an excellent option for situations where a more involved procedure is not feasible or contraindicated. Furthermore, the resulting wound at the donor site is rarely an issue for the patient or their caretakers.
Pinch grafts are useful for large wounds that would benefit from second intention healing, but would take an extended period of time to heal without a reconstructive assist. Patients with a history of slow-healing wounds on the scalp or lower legs by second intention may benefit from pinch grafting. A patient unwilling or unable to tolerate a more extensive or prolonged procedure similarly may benefit from the very brief period of time required for harvest of pinch grafts.
If there are concerns about the patient’s ability to care for wounds, pinch graft donor site wounds are at low risk for postoperative complications and are very easy to care for. Over the long term, skin quality—including thickness, durability, and pigmentation —is closer to a FTSG than an STSG. Initially the grafted areas often display a cobblestoning effect, which improves with time.
The technique involves a scalpel or razor blade and forceps, and pinch grafts are typically 4 to 10 mm in size. The most common donor site is the anterior or lateral thigh, though skin overlying the clavicle or mastoid, or even the tissue surrounding the defect if definitively cleared with Mohs surgery, are also appropriate donor sites.
After prepping the donor site, circular or oval, partial-thickness shave excisions are performed (Fig. 44-13). The thickness of the grafts may be variable, as thinner graft donor sites heal more quickly and the grafts themselves have lower metabolic requirements. With these characteristics in mind, a tangential excision of a thickness ranging from less than a millimeter to 2 mm can be obtained. Local anesthetic infiltration of the donor site skin immediately prior to harvesting causes increased turgor, permitting the graft to be immediately, tangentially excised before the swelling subsides. The graft is transferred to the wound or kept on saline soaked gauze while
subsequent grafts are harvested. The number of grafts needed varies based on the size of the wound and the goals of reconstruction. However, for small- to moderate-sized wounds, placement of the grafts within 1 cm of the scalp wound margin and then spacing them 5 to 10 mm apart is the usual grafting pattern. Once all grafts have been placed, the recipient wound is very carefully covered with petrolatum gauze. Care is taken to not displace the grafts during bandaging as they are not sutured into place. The goal is to immobilize the wound, and the grafts will become adherent to the wound within a few hours. Once covered with gauze, a bulky dressing is applied over top and normally affixed and immobilized through adhesive taping. If there is concern about the security of a taped bolster, a tie-over bolster dressing is reasonable and will assure immobilization of the graft. No additional wound care is needed and the donor sites are cared for with standard occlusive wound care. The patient returns in 1 week for careful removal of the dressing. The wound bed and margins are gently cleansed with water and petrolatum gauze is reapplied with a clean bulky dressing and left in place for one additional week. Thereafter, standard, daily occlusive wound care is initiated until healing is complete. The islands of epidermis and dermis quickly begin to expand and coalesce over the next few weeks until reepithelialization is complete. For large wounds, a second session of grafts is occasionally helpful to further expedite healing.
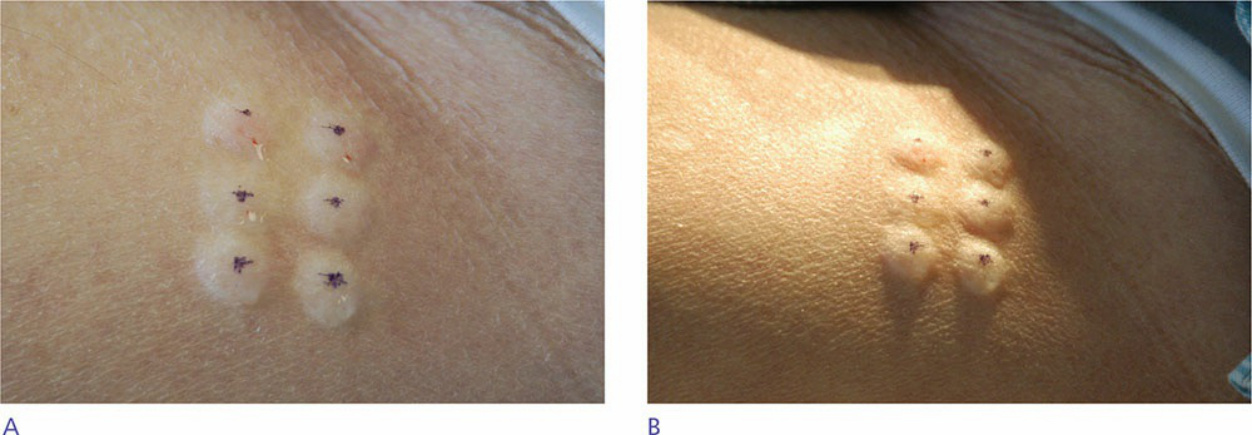
Figure 44-13. (A) Pinch graft donor site after superficial infiltration with local anesthesia. (B) Side lighting shows the swelling from local anesthesia which makes pinch graft harvesting simple.