Split-thickness skin grafts
Split-thickness skin grafts
STSGs have special attributes that may be beneficial in the repair of scalp wounds. Their advantages include a low metabolic requirement for engraftment, leading to higher rates of graft survival. Large wounds can be covered, since harvesting large grafts is relatively simple (Fig. 44-11). Donor site wound care is straightforward, as it is managed by standard occlusive wound care technique. STSGs diminish the immediate postoperative risks of bleeding and the more long-term risk of delayed wound healing compared to wounds allowed to heal by second intention. Wound care of the graft itself is relatively simple for the patient, since the bolster dressing remains in place for 7 days, after which a second bandage is applied for the second week. Thereafter, the well-healing graft is kept moist with daily application of ointment or moisturizers.
There are also disadvantages inherent to the STSG. First, they are by definition partial-thickness skin replacements that are used for full-thickness skin loss. Therefore, both the aesthetics of the repair and the durability of the healed skin may be suboptimal (Fig. 44-12). Often, a healed STSG remains depressed below the natural contour of the surrounding scalp, and the grafts typically become hypopigmented and have no appreciable texture or adnexae. STSGs mandate the creation of a second wound necessitating several weeks of wound care. Donor wound sites are often painful initially and, on occasion, are complicated by postoperative bleeding. The wounds also generally heal with a hypopigmented scar. They rarely become hypertrophic because of their very superficial nature. Another potential disadvantage of STSG is the requirement for a mechanical device for harvesting, requiring set up and technical training.
There are three fundamental methods of STSG harvesting. The first is freehand harvesting by the surgeon using a scalpel or razor blade held tangentially to the skin. This technique is effective for smaller grafts, though, they are typically thicker and more variable in thickness than those harvested using a device. The other two techniques involve using a separate device. These include nonmotorized devices such as the Weck blade, or motorized dermatomes such as the Paget or Brown dermatome.
Weck Blade Technique The Weck blade includes a handle with a single-edged blade and a blade guard designed to produce grafts of varying thicknesses. The thicknesses typically range from 0.08 to 0.18 in. The blade guard is approximately 4 cm in width and, as a result, grafts up to approximately 3 cm can be easily harvested.
Potential Weck blade donor sites include the skin overlying the mastoid process, the occipital scalp, the clavicle, and the mid to upper anterior or lateral thigh. The scalp donor site rapidly reepithelializes due to the high density of hair follicles, and is often used repetitively as a donor site in burn victims. The mastoid process and clavicular skin are excellent sources of skin, and the underlying bony structure makes the harvest easier for smaller grafts. The convex surface of these areas also makes more precise sizing of the graft easier. On less rigid surfaces such as the thigh, it is helpful for both the surgeon and assistant to retract in opposite directions along the direction that the graft will be harvested, compressing the soft tissue by squeezing deeply to increase the convexity of the donor skin during graft harvest. This permits the width of the graft to be easily varied by the surgeon. A wider graft will be obtained with more downward pressure placed on the Weck blade, and a narrower graft is harvested with less downward pressure. Training and experience are very beneficial, and result in more precisely shaped and sized grafts.
The technique for the Weck blade harvesting begins with prepping the skin and local infiltration of the skin with anesthetic. The area to be harvested can be marked or templated and prescored with a scalpel using the template. Once the donor site is prepped, the skin is lubricated with mineral oil, nontoxic soap, or ointment. The device is placed at one end of the donor site and angled at 30 degrees to the skin. Constant downward pressure is applied to the blade throughout graft harvesting. The surgeon’s nondominant hand is then placed on the opposite side of the donor site and traction is applied away from the Weck blade device. When the donor site is a softer area such as the thigh, it is helpful to have an assistant providing countertraction in the opposite direction of the surgeon’s hand. The graft is then harvested using a back and forth sawing motion of the device, which is kept at a 30-degree angle to the skin throughout the procedure. Once graft harvest begins, it must continue until the graft is entirely harvested as it is not possible to reposition the blade and resume harvesting once the blade has been lifted from the skin. Upon complete separation of the graft, the Weck blade is pulled back in the opposite direction, and the graft is severed at the terminal end of the donor site by a scalpel or scissors. The graft is then cleansed to remove lubricant and transferred to the wound.
Once transferred, care is taken to ensure that the undersurface of the graft is in contact with the wound base and the graft is gently unfolded and distributed across the wound. It can then be tacked into place and trimmed to fit the wound.
Once circumferentially sutured, the graft can be further secured to the wound base either by tacking sutures or tie-over bolster dressings. Vaseline impregnated gauze is also useful and can serve as both a nonstick surface and bulk for bandaging.
Motorized Dermatomes Motorized devices such as the Paget or Brown dermatome are also useful for harvesting
STSGs of precise thicknesses. The blade guard width and thickness is often adjustable, making these devices customizable. The maximum width of the graft varies between machines, but is generally larger than the Weck blade. As such, the usual donor site is the mid to upper anterior or lateral thigh. Again, once graft harvesting begins, it cannot be suspended and restarted. Upon separation of the graft, the dermatome is withdrawn and the graft is detached with scissors or scalpel. The graft and dressing are applied as above.
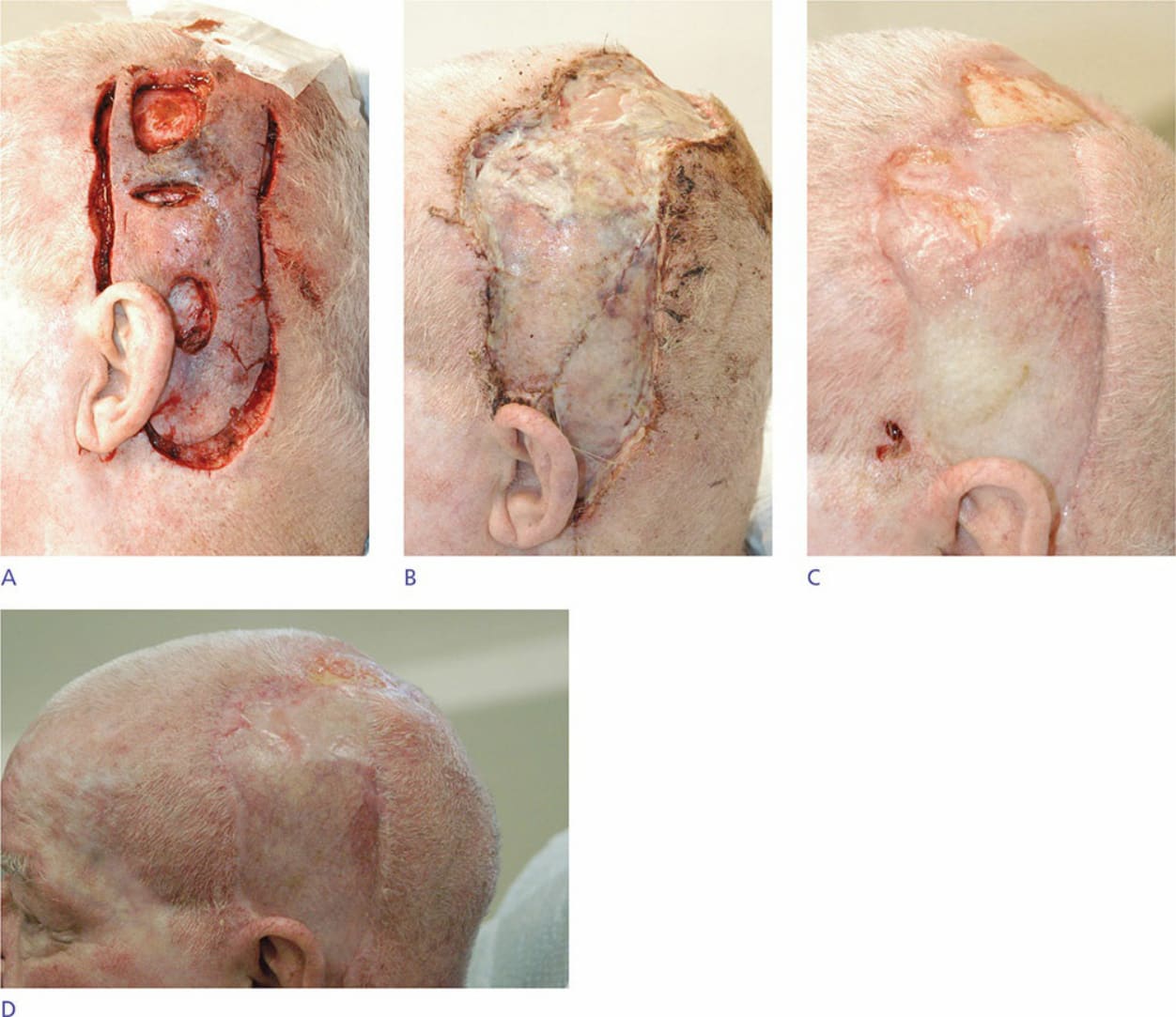
Figure 44-11. (A) Preoperative excision of large infiltrative squamous cell carcinoma. (B) Two weeks after placement of split-thickness skin graft harvested from the anterior thigh. (C) Six weeks postoperatively. (D) Three months postoperatively.
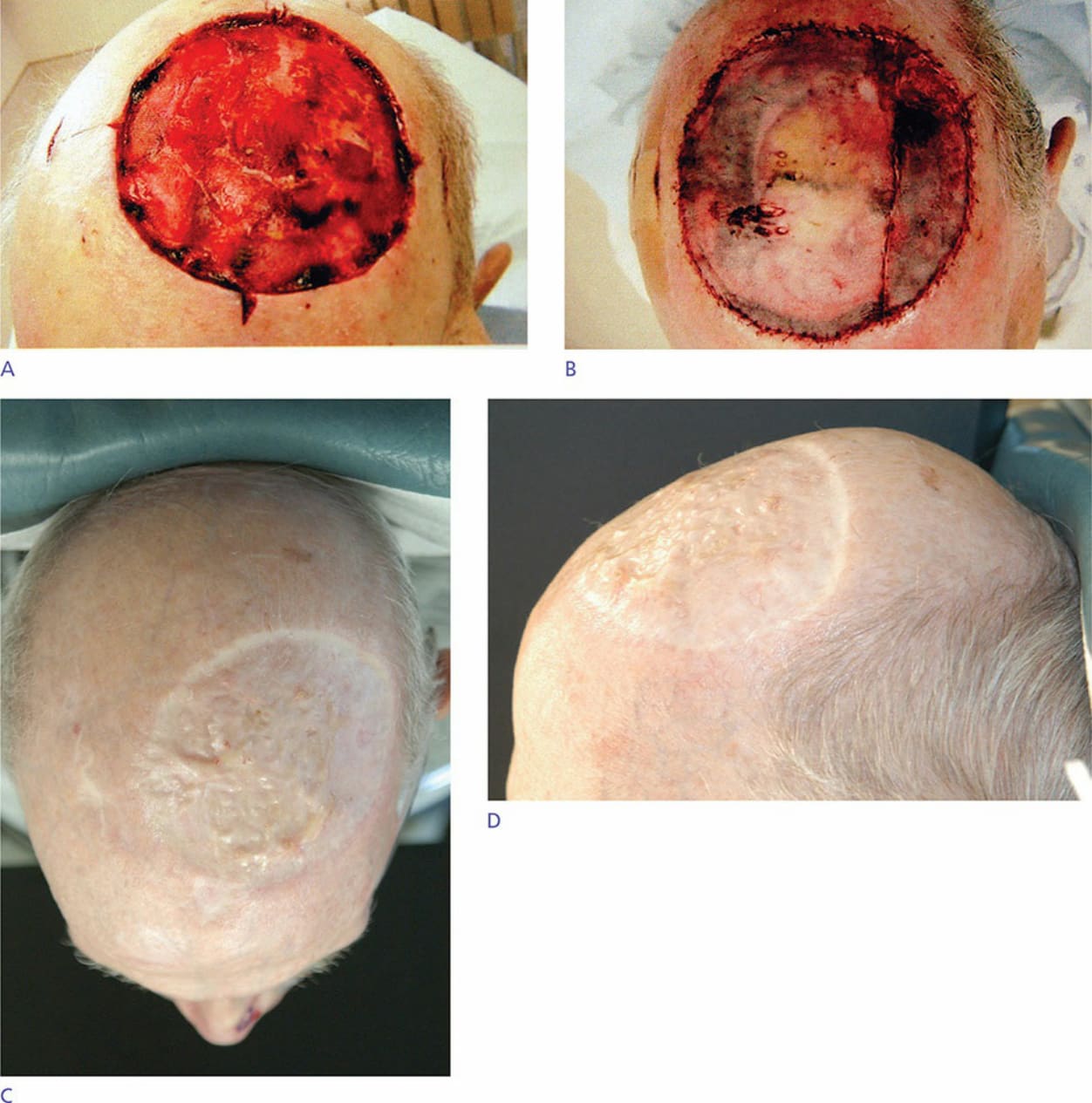
Figure 44-12. (A) Postoperative defect after Mohs excision of microcystic adnexal carcinoma of the left frontal and parietal scalp. (B) Large split-thickness skin graft sutured into place. (C,D) Follow-up at 2 years.