Full-thickness skin grafts
Full-thickness skin grafts
FTSGs are often very effective for reconstruction of the scalp (Fig. 44-10). Although they do not replace hair, they may be highly aesthetic for reconstruction of a bald or balding scalp. Results following full-thickness graft procedures may be durable, and are accomplished with relative ease (Table 44-5).
The FTSG procedure begins with identifying the most appropriate donor site, which may be any area with sufficient laxity to permit closure following graft harvest. Consideration of thickness, quality, and textural match of the scalp skin is important. The most readily available donor site with excellent tissue match is the supraclavicular fossa. This area provides ample donor skin, which is relatively thick, durable, and elastic, and tends to match scalp skin well, especially in the bald scalp. A template is made of the defect and used to precisely score the donor skin surface. Typically, a 90- degree incision to the fat is made along the score line. Upon removal, the fat is trimmed from the undersurface of the graft with scissors. The graft is then placed in the wound, tacked into place, and circumferentially sutured into the wound.
There are several simple principles that optimize the chances for complete survival and cosmesis of a graft. The first of these is to obtain a correctly sized graft. Oversizing the graft is not recommended as the texture and turgor of the engrafted tissue will not appear normal. Similarly, a graft that is undersized may be too thin, or may result in tension-related graft necrosis at the margins. For these reasons, a template is made of the wound and used at the donor site to precisely incise a correctly sized graft.
The second key principle is ensuring that the graft is immobilized and remains in contact with the wound base during the first week to optimize the inosculation phase of engraftment. This can be accomplished with either quilting sutures or a bolster dressing. The graft can be quilted to the underlying wound base by absorbable sutures placed through the undersurface of the graft and then into the corresponding area of the wound base. Alternatively, these sutures can be placed through the surface of the graft into the wound base after the graft has been sutured. Both techniques serve to affix and secure the graft to the wound base. Alternatively, a bolster dressing is perhaps the simplest method to maintain complete contact of the graft to the wound base. This can be accomplished by covering the graft with nonstick gauze followed by fluffed gauze. Sutures are then placed across the bolster from one side of the wound to the other. Larger wounds may require several of these crossover sutures to ensure adequate and evenly distributed compression of the graft against the wound base. Regardless of the method, the essential principle of these techniques is to ensure that the wound base and graft remain immobilized and in contact with the wound without shearing motion during the early phase of engraftment. Any part of the graft that is not in direct contact with the vasculature of the base will not survive.

Figure 44-10. (A) Post Mohs excision of basal cell carcinoma of the left vertex. (B) Full-thickness skin graft placed. (C) Two months postoperative with excellent healing of the graft which is inconspicuous because of adjacent hair regrowth.
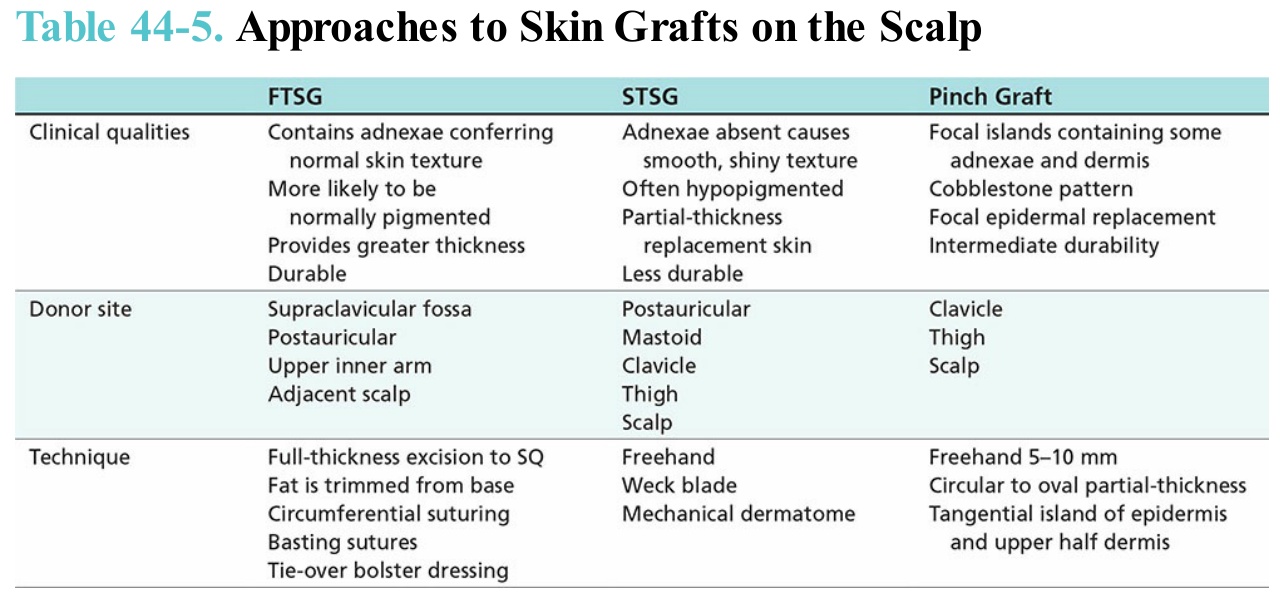
Table 44-5. Approaches to Skin Grafts on the Scalp