Second intention healing
Second intention healing
The simplest approach to scalp wound management is wound closure by second intention. As such, it is important to understand the relative and occasionally absolute indications and contraindications for selecting this option (Table 44-3).
The first step in selecting second intention wound management is patient education (Fig. 44-2). If the patient indicates a preference for allowing the wound to heal by second intention and there are no contraindications, then this option is an excellent choice. When the scalp is scarred from previous procedures or injury, or if it is completely inflexible, second intention wound healing should also be considered. When the adjacent tissue that would be used for the primary closure is unacceptably compromised either from severe actinic damage, other skin cancers, or inflammatory conditions such as erosive pustular dermatosis, then healing by second intention becomes an ever more attractive option.
There are additional occasions when circumstances favor less surgery, such as in a combative patient with dementia who is expected to or known to remove bandages and excoriate or mutilate the wound. If for any reason it is in the patient’s best interest to delay primary closure, or if the decision to perform primary closure cannot be made at the time of surgery, second intention wound healing is preferred.
Relative contraindications for second intention wound healing include cases where primary closure would be technically straightforward and would shorten the time to healing. A closed wound in a patient with known thrombophilia or who is on anticoagulants may be preferable to reduce the chance of postoperative bleeding. Some patients with a known tendency for extremely prolonged wound healing of the scalp should also be considered for primary wound closure. Second intention wound healing is typically more labor intensive for the patient and, if their social support situation is not conducive to adequate wound care over prolonged periods of time, second intention
wound healing may be impractical. Similarly, this approach is inadvisable when patients are undergoing chemotherapy, are neutropenic, or have compromised wound healing. Thus careful consideration of the patient’s health, social situation, and other unique nuances may assist in the decision regarding second intention wound management.
Second intention healing and ancillary augmentation techniques
Optimizing wound care is of vital importance once a decision to allow the wound to heal by secondary intention is made. Adjustments in the routine wound care may need to be made based on the details of both the health of the patient and the nature of the wound, though typical wound care consists of daily bandage changes and very gentle cleansing of the wound (Table 44-4). The basic bandage is a nonstick dressing placed over the ointment-covered wound base and affixed with adhesive tape, if possible.
Daily bandage changes are performed carefully to avoid injury to the newly formed epithelium growing in from the margins. Likewise, cleansing of the wound itself is performed gently with tap water. If the patient showers daily, cleansing can be
conveniently done in the shower. After several weeks, in a normally healing wound, every other day bandage changes may be feasible and even beneficial by lessening incidental trauma to the regrowing epithelium. Similarly, hydrocolloid dressings can be substituted for daily dressing changes once the wound becomes less suppurative, generally after 2 to 3 weeks. These bandages may be left in place for up to 7 days and are most feasible on bald scalps. They should only be used if they can be kept on the wound for at least three consecutive days.
Scalp wounds are sometimes treated with topical antibiotic ointments, such as mupirocin. With longstanding wounds (over 1-month duration), prophylactic anticandidal ointment may be added to mitigate the risk of yeast overgrowth.
Ancillary techniques are available to augment and abbreviate second intention healing. These include reducing the size of the wound with partial closure, and covering or filling the wound with skin substitutes that may enhance and stimulate healing.
The simplest wound augmentation technique is reducing the size of the defect with sutures (Fig. 44-3). If a wound cannot be reduced in diameter by 50% or more, the degree of benefit from partial closure diminishes.
Partial closure may be effected in several ways. The first is placement of buried horizontal mattress sutures across the wound (Fig. 44-4). Scalp dermis is variable in its tensile strength and is occasionally fairly atrophic. Densely hair-covered dermis is also often less able to withstand high-tension suture placement. The order of suture placement may have an impact on closure success (Fig. 44-5). Placement of the first suture on one end of the wound, and working along the wound to the other end will allow greater approximation of the wound, using a zipper-like effect.
Another technique for wound approximation involves the use of a pulley or double suture technique. Several variations of this approach are possible, including the
mechanically advantaged suturing technique with a series of four horizontal mattress sutures where the suture material loops in the center (Fig. 44-6), but all confer the mechanical advantage of a pulley that ultimately permits better tissue movement.
Another helpful technique to reduce the overall size of scalp wounds is the pursestring suture (Fig. 44-7). Once all sutures are placed, the wound edges are pulled centripetally together, though without mechanical advantage. Various other techniques, such as the guitar-string suture technique, are available as well.
Another way to augment second intention wound care is with epidermal or dermal substitutes. They may be used in wounds partially closed with one of the aforementioned suturing techniques, or independent of any previous wound closure. These skin substitutes effectively provide a covering to the wound base and may induce more rapid granulation and healing. Secondary benefits of these products include improved hemostasis and exudate control postoperatively, less burden on the patient for wound care, and some protection of the wound base from external factors.
Epidermal substitutes, most typically porcine xenografts or cultured epithelial autografts, function to induce and enhance granulation tissue formation (Fig. 44-8). The placement of the xenograft is technically straightforward, and entails simply trimming it to the size of the defect or, in larger wounds, placing multiple xenografts over the base of the wound in a patch-work fashion. In wounds that are partially closed, the xenograft can be inserted beneath the sutures. Thereafter, nonstick gauze is placed over ointment, and a bolster dressing is applied. After bolster removal 1 week later, daily to every other day, bandage changes are initiated using standard occlusive wound care. The xenograft can be debrided in 3 to 4 weeks, and standard occlusive wound care is continued until healed or, alternatively, delayed FTSG can be considered.
Dermal substitutes may also be placed into the wound, and can be held in place with sutures or overlying dressings for up to a week. Thereafter, standard occlusive wound care can be initiated. Unlike xenografts, it is expected that the dermal skin substitutes will become incorporated into the wound, and therefore debridement is not necessary.
Dermal skin substitutes may also be beneficial in very deep wounds. These products are generally used to replace the full-thickness of skin and improve the quality of the scar once healed. These are left in the wound to be incorporated in the healing process. Some are bilayered with a deep bovine collagen and glycosaminoglycan dermal layer and an overlying silicone sheet which must be removed at approximately 3 weeks. This can be an elegant way to speed healing dramatically. These products may be costly however, and are reliant on an adequate vascular base.2
Defects that extend to bone, where periosteum is no longer present, may not readily form granulation tissue. When failure to form granulation tissue is confirmed, cautious chiseling of the outer table of the bone using a bone chisel and mallet may effectively expose a vascular supply derived from the bone and facilitate formation of granulation tissue. After partial removal of the outer table, pinpoint bleeding is observed signifying accomplishment of the goal. Less than 1 mm of the outer table is typically removed (Fig.
44-9). The chiseled area is then immediately covered with ointment and occluded using standard occlusive wound care. An alternative to standard occlusive wound care for these wounds is the use of a hydrocolloid dressing changed every 7 days. Granulation tissue formation tends to be more rapid and exuberant with these dressings in slow-toheal, desiccated wounds. Buds of granulation tissue are expected within a few weeks and they continue to proliferate, ultimately creating a vascular base that can then be resurfaced either with a delayed graft or naturally by marginal reepithelialization.
Recent reports of air embolism after chiseling the outer table of the bone underscore the caution necessary for this procedure. If chiseling of the outer table is deemed necessary, it should be performed with the patient in a flat or reverse Trendelenburg position, and the wound should be immediately and completely occluded with ointment and bandages. The reverse Trendelenburg position decreases the chance of negative pressure formation at the chiseled surface, which can draw air into the vascular system and create air emboli. Likewise, immediate occlusion serves to seal the vascular
channel and diminishes the chance of this complication. Nonetheless, this technique should not be utilized without due consideration of these potentially serious complications.

Figure 44-2. (A) Preoperative melanoma of the scalp. (B) Post Mohs defect. Patient expressed strong preference to allow the wound to heal by second intention. (C) Partial closure reducing area by >50%. Wound is packed with gel foam. (D) Long-term follow-up with acceptable result.
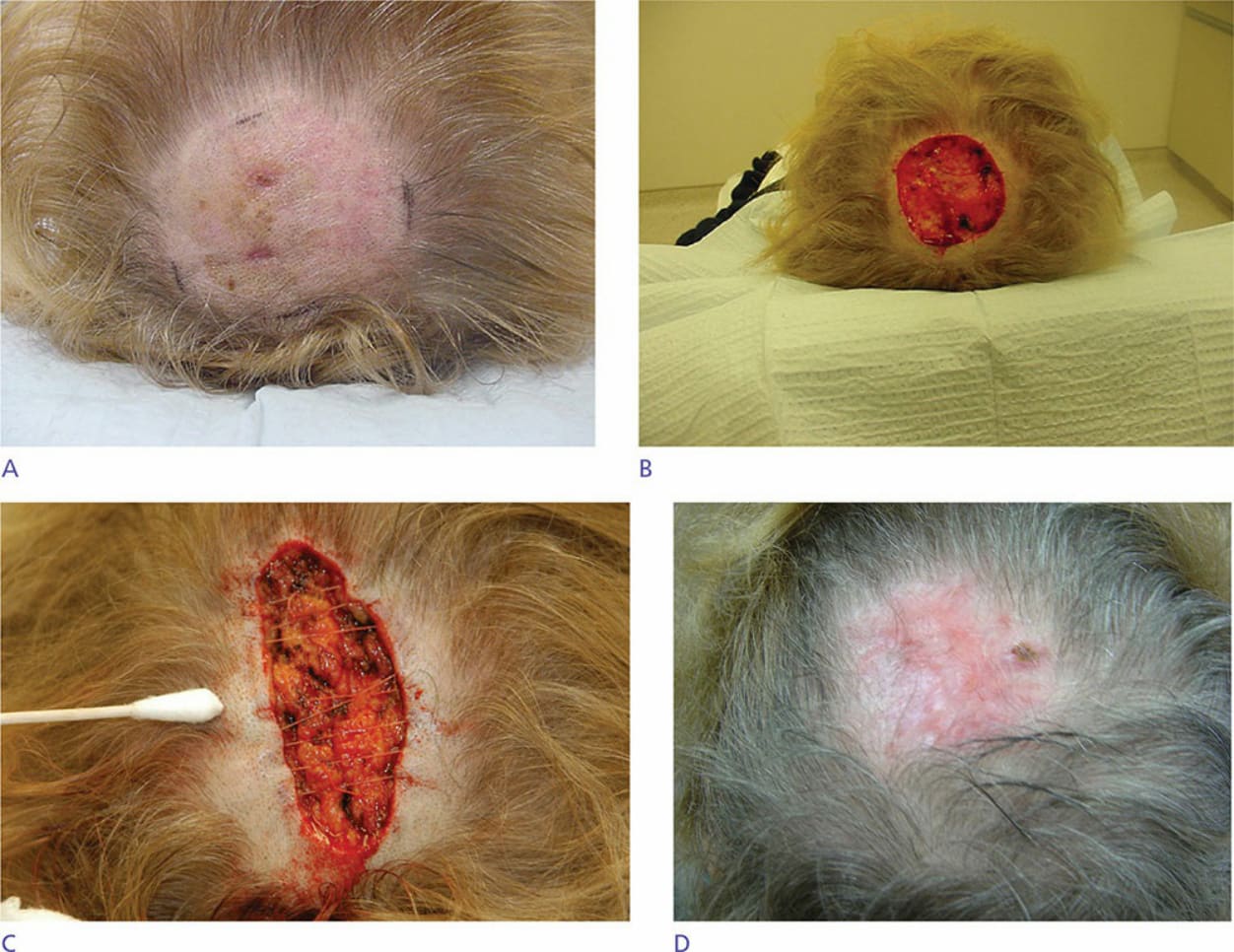
Figure 44-3. (A) Large melanoma of the vertex scalp. (B) 7.5-cm defect post Mohs surgery. (C) Greater than 50% reduction of wound by a combination of mechanically advantaged suture technique and dermal horizontal mattress sutures. (D) Healed wound 2 months postoperatively.

Figure 44-4. (A) Large defect after Mohs excision of squamous cell carcinoma. (B) Partial closure of defect and substantial reduction of remaining wound with buried horizontal mattress sutures. The resulting wound is allowed to heal by second intention. Wound was packed with gel foam.
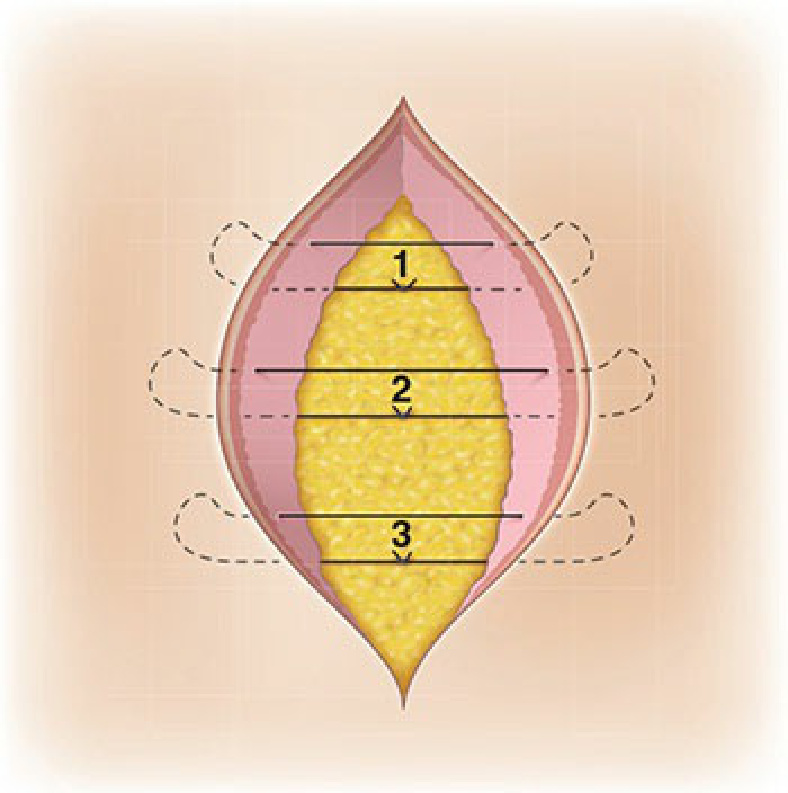
Figure 44-5. Order of suture placement for ease of technique.
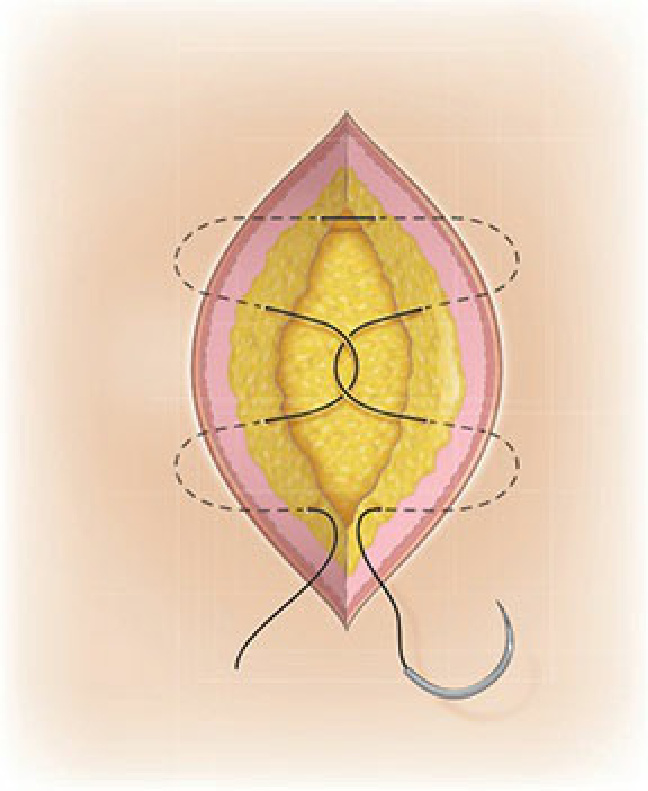
Figure 44-6. Diagram of mechanically advantaged suture technique which consists of four buried horizontal mattress suture bites with a central interlocking suture which forms a dynamic pulley system. The pulley provides a 2:1 mechanical advantage.
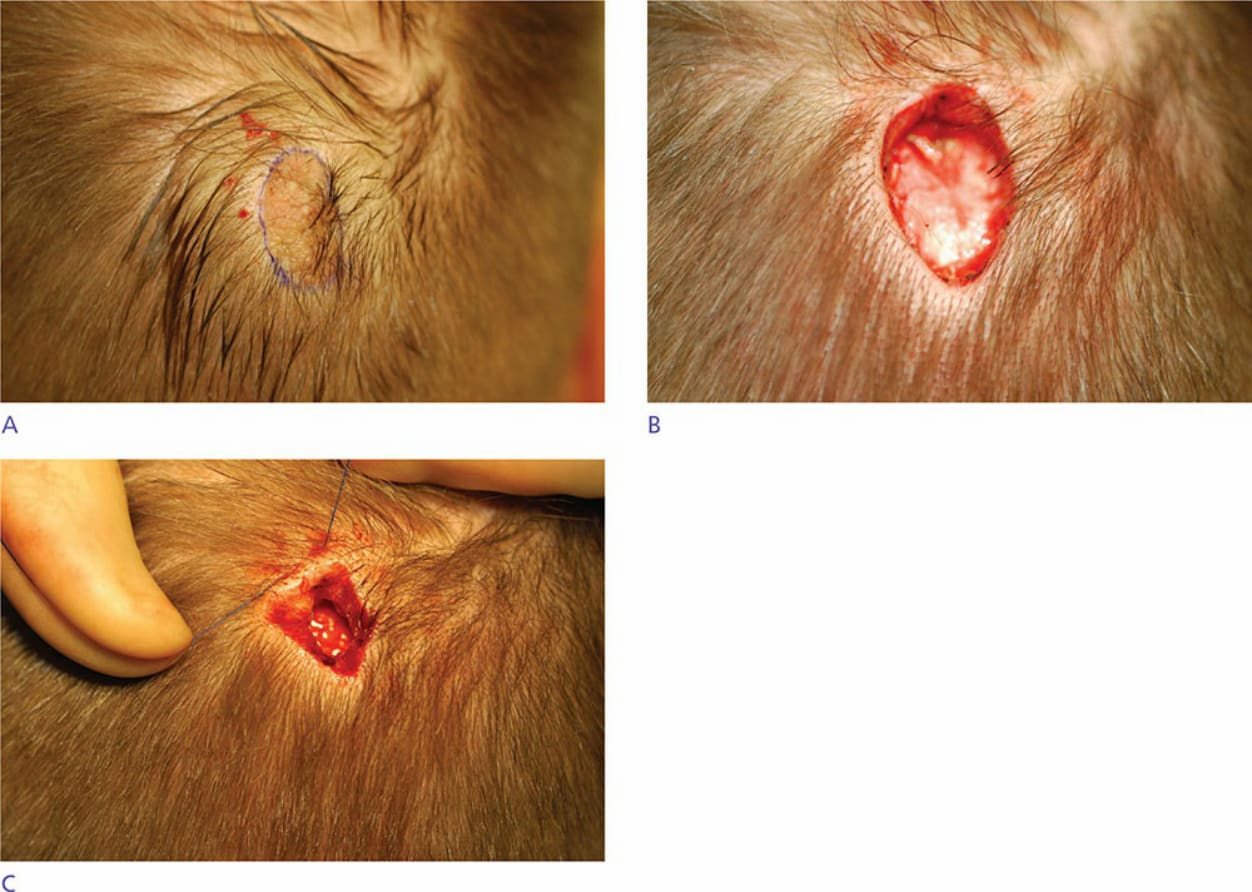
Figure 44-7. (A) Preoperative excision of basal cell carcinoma arising within a nevus sebaceous. (B) Postexcision of tumor. (C) Substantial diminution of defect using purse-string suture technique.
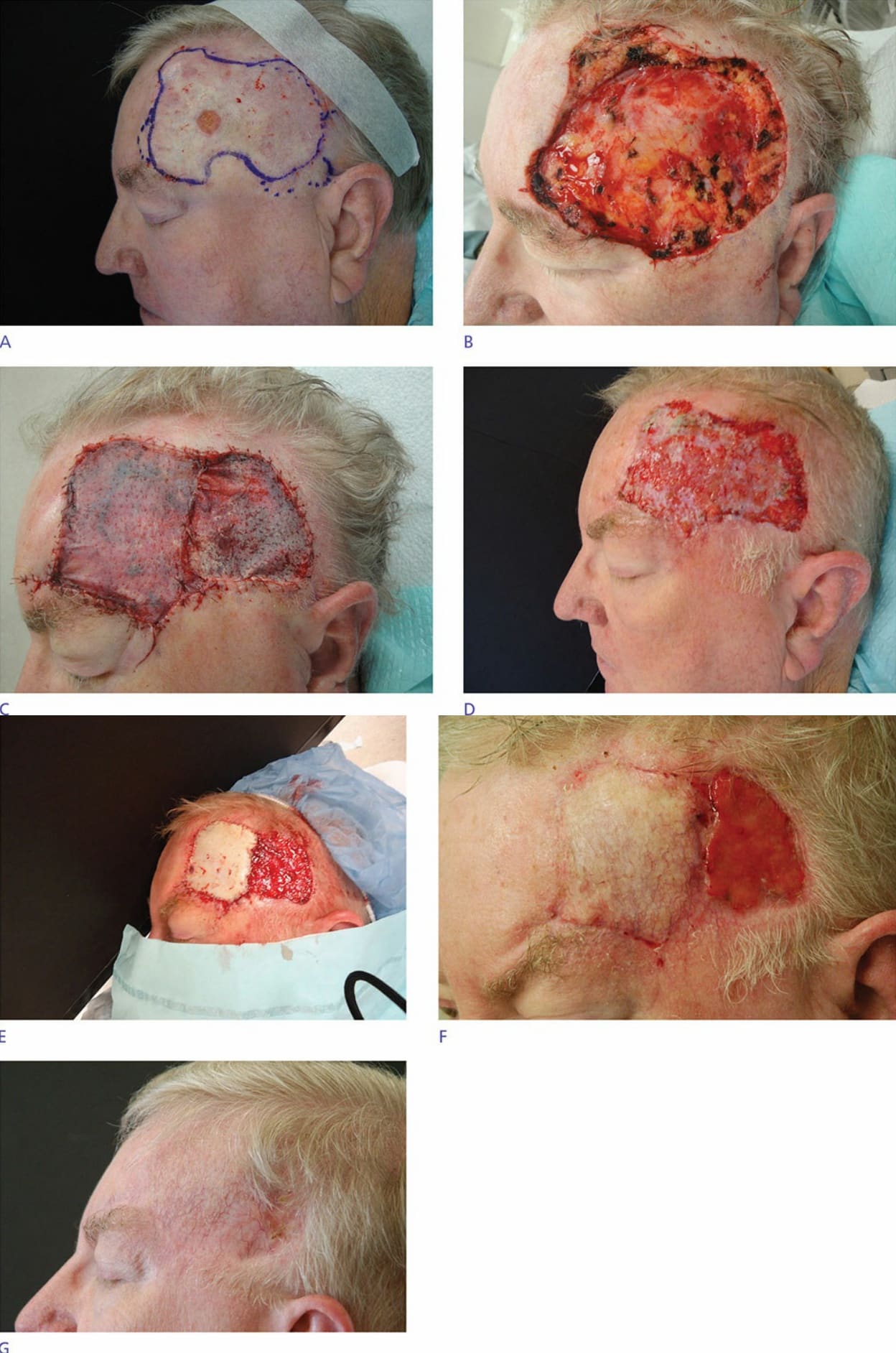
Figure 44-8. (A) Large basal cell carcinoma of the left temporal scalp and temple preoperatively. (B) Post Mohs excision defect. Some follicles were preserved in the posterior temporal scalp wound. (C) Preliminary coverage with xenografts over the entire wound to induce more rapid granulation of the wound. (D) Three weeks postoperatively xenograft debrided exposing excellent granulation tissue. (continued)

Figure 44-9. (A) Preoperative multiply recurrent basal cell carcinoma. (B) Post Mohs excision requiring removal of periosteum as well as a bone layer using decalcification techniques with micrographic surgery. Denuded portions of the bone have been chiseled to pinpoint bleeding. (C) Six weeks postoperatively with excellent early granulation arising from exposed bone. (D) Three months postoperative with complete granulation coverage of exposed bone. The wound went on to heal entirely by second intention.
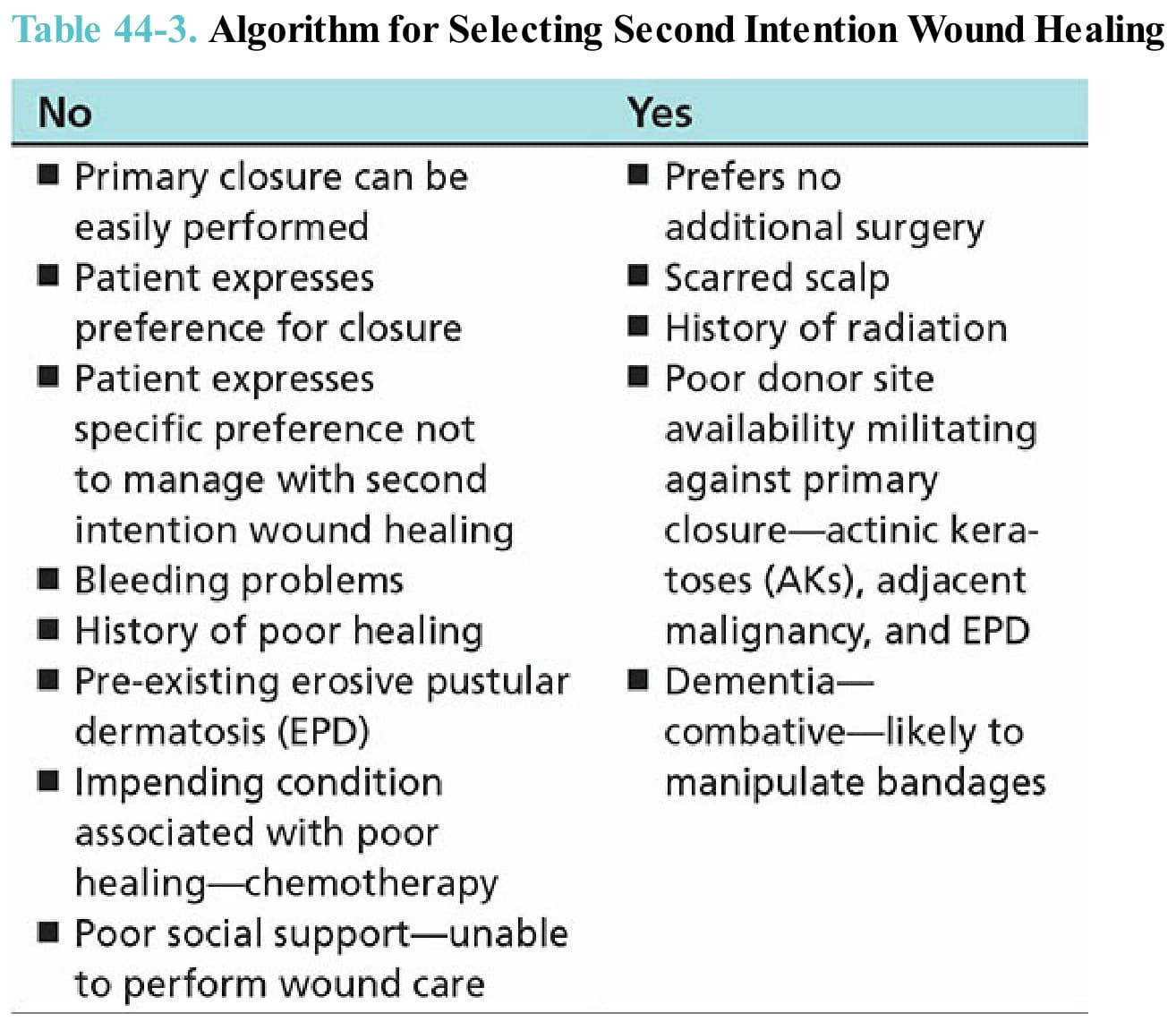
Table 44-3. Algorithm for Selecting Second Intention Wound Healing
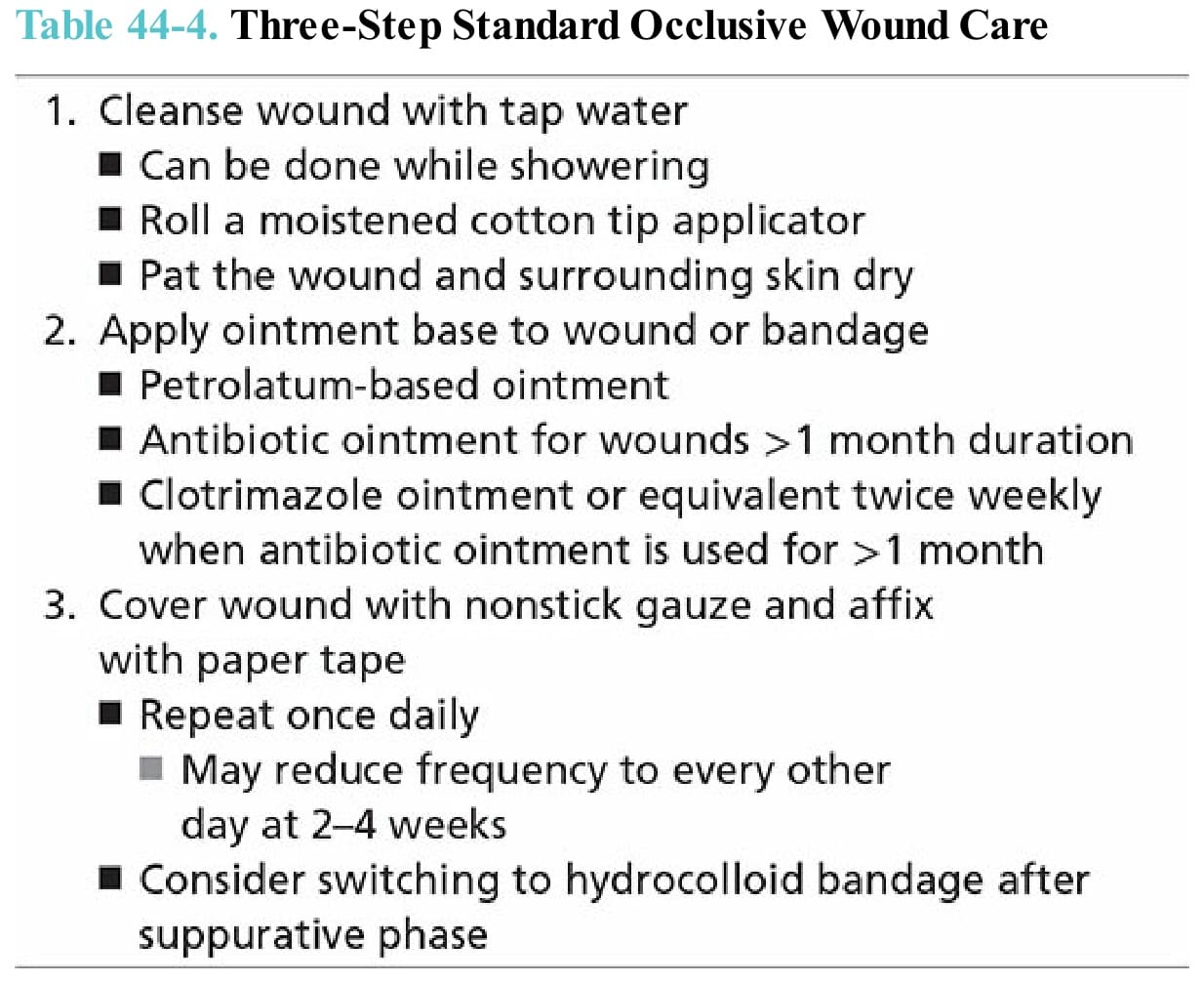
Table 44-4. Three-Step Standard Occlusive Wound Care