GENERAL CONSIDERATIONS
GENERAL CONSIDERATIONS
The scalp has several unique characteristics that may dictate decisions for optimal wound management. First, there is a diverse level of aesthetic concern among patients: A surprising number of patients have a low level of concern regarding scalp appearance, particularly when compared to more visible areas of the face such as the nose, cheeks, or lips. Therefore, wound management is often profoundly influenced by the aesthetic expectations of the patient (Table 44-2). Furthermore, function is rarely a concern for the scalp, and so a substantial proportion of patients are content to simply camouflage otherwise noticeable scars with adjacent hair.
Another unique characteristic of the scalp is that hair-bearing skin heals nicely without any reconstruction if the wound can safely be kept superficial enough that the hair follicles are preserved and can regrow. As the hair regrows, it may completely camouflage a scar that would otherwise be noticeable in non–hair-bearing skin (Fig. 44- 1).1
Scalp skin is among the thickest of the body; it is inelastic, immobile, and difficult to work with during reconstruction. It typically has limited reservoirs of adjacent lax skin to be used as donor skin. Paradoxically, despite its thickness, one of the scalp’s unique features is that the dermis is often relatively thin or lacks the tensile strength necessary to withstand the very high tensions that may be needed to suture wound edges. Bald scalp dermis is frequently thinner than expected, while hair-bearing skin lacks durability and may tear under high tension with large gauge sutures due to the high follicular density. These characteristics vary dramatically from person to person, and must be carefully assessed prior to planning the reconstruction.
The importance of complete removal of a skin cancer of the scalp cannot be overemphasized. Aggressive and metastatic scalp tumors may be a function of the abundant blood supply of the scalp or the greater likelihood of delayed diagnosis. There is a tendency to remove tumor with narrower margins than recommended when performing a standard excision, likely given the challenge that an immobile and inelastic scalp wound poses for closure. Therefore, the tissue sparing qualities of Mohs micrographic surgery may be particularly useful on the scalp. Furthermore, safely removing tumor with relatively superficial depth is enabled by Mohs surgery, which may obviate the need for reconstruction entirely if the wound can be allowed to heal by second intention.

Figure 44-1. (A) Second intention wound scar 1 year postoperative after suprafollicular tumor excision. (B) Regrowth of hair through scar provides excellent cosmetic result.
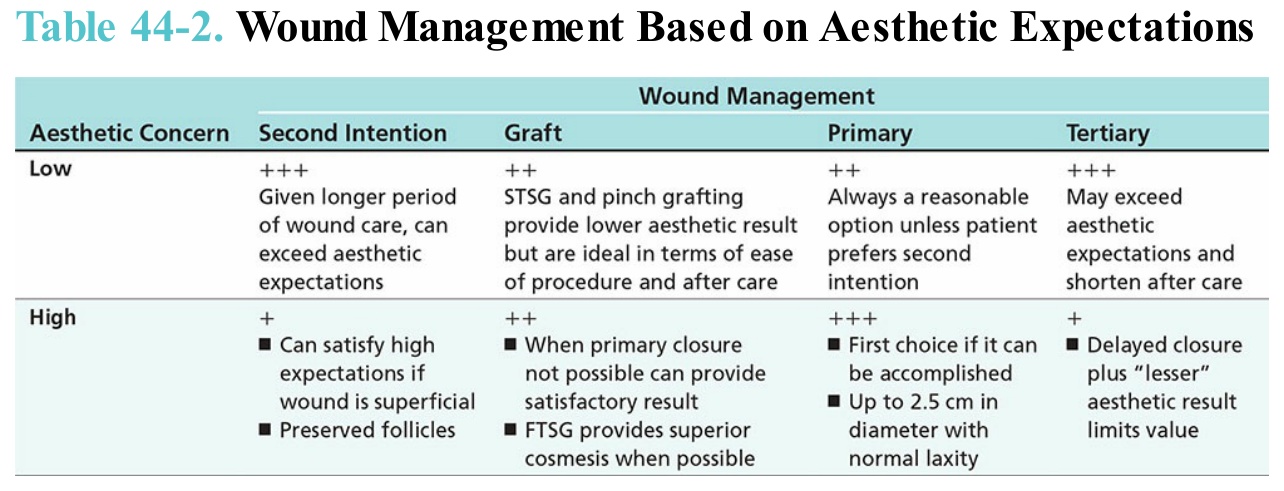
Table 44-2. Wound Management Based on Aesthetic Expectations