Eyebrow Reconstruction
Eyebrow Reconstruction
Just as the planning of forehead and temple defect repairs centers around the maintenance of eyebrow positioning and symmetry, reconstruction of the eyebrow subunit itself similarly requires close attention to eyebrow continuity, shape, and positioning.
Second intention healing should be reserved for those defects that are small and extend only into the superficial dermis, so that maintenance of hair regrowth from the hair bulbs can occur. Full-thickness defects will require layered closure, and primary closure remains the mainstay approach for small- to moderate-sized defects. Defects located immediately adjacent to the eyebrow superiorly or inferiorly may be closed with a horizontal arciform primary closure, and hide well along the eyebrow margin (Fig. 43-36). Careful planning may assure that eyebrow closures do not place excessive vertical traction of the upper lid prior to excising the standing cones for primary closure, and that sufficient eyebrow height remains so as not to create eyebrow asymmetry (Fig. 43-37).
Defects with wider horizontal dimension may also be closed primarily in a vertical fashion, and the remaining eyebrow should be marked with a surgical marker prior to local anesthetic infiltration to facilitate ideal alignment and minimize eyebrow distortion. As the eyebrow represents a free margin, vertically oriented primary closures have the tendency to bulldoze the eyebrow and upper eyelid inferiorly upon closure. Therefore, it may be helpful to displace the inferior standing cone deformity across the arc of curvature as it traverses the orbital rim and upper lid. This acts to diminish the degree of tissue pushed inferiorly, as tissue redundancy dissipates over the convexity of the upper eyelid in the manner of a crescentic advancement flap (Fig. 43- 38). Medial eyebrow defects may be repaired with vertically oriented closures, as the glabellar crease camouflages the resultant scar (Fig. 43-39).
Larger defects in or adjacent to the eyebrow often necessitate adjacent tissue transfer for reconstruction or to minimize deformity of the residual eyebrow. Advancement
flaps, whether unilateral or bilateral, are the mainstay of eyebrow reconstruction, as the majority of the incision profile may be hidden along eyebrow margins. Similarly, advancement flaps offer great utility in minimizing subsequent eyebrow removal or displacement in individuals with sparse eyebrow hair (Fig. 43-40). Flap design along the eyebrow subunit almost always involves elements of both advancement and rotation, which are required to hide incisions along the arc unique to an individual’s eyebrow (Fig. 43-41). As with all facial reconstruction, displacement of scar contours or profile laterally allows visual subtraction and a more aesthetically pleasing repair (Fig. 43- 42). Both A-to-T and H-plasty variations may all be useful advancing flaps within the eyebrow. V-to-Y flaps offer the additional benefit of moving a residual hair-bearing island on a well-perfused deep vascular pedicle into alignment with the remaining medial eyebrow (Fig. 43-43).
Wider defects of the lateral eyebrow may require transposition flaps for recruitment of tissue to fill the defect. In such cases, the repair may not reintroduce eyebrow hair, but instead attempts to minimize lid contraction postoperatively, and diminish the risk for ectropion formation (Fig. 43-44). In surgical repairs that do not preserve or recreate eyebrow hair, transplantation may be performed in the postoperative period. The occipital neck and sideburn are both potential donor sites which may serve as good matches for the residual eyebrow.12,13
CONCLUSIONS
Reconstruction of the forehead and eyebrows is frequently performed by dermatologic surgeons. As with all reconstructive approaches, linear repairs may be the most straightforward, though flaps are often necessary in order to restore normal anatomical form and function. Appropriately orienting linear closures, and wisely selecting from an array of flap repair choices, may help create the ideal closure for the patient and minimize the risk of functional or cosmetic compromise.
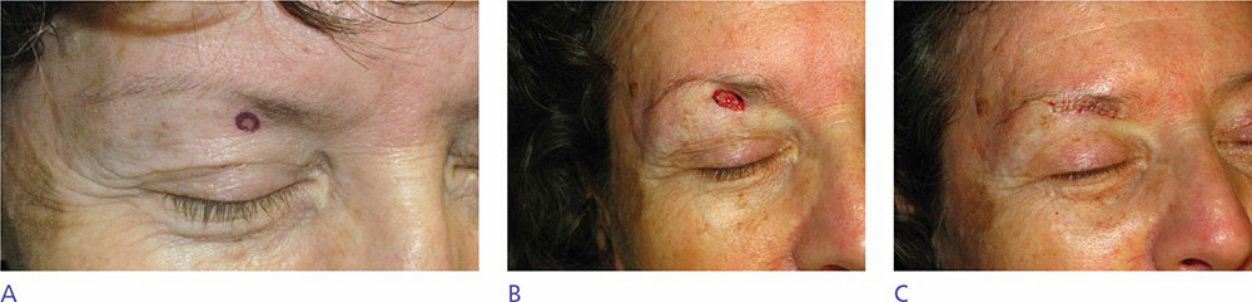
Figure 43-36. (A) BCC of the right mid inferior brow. (B) A 1.1 × 0.7 cm full-thickness defect of the right mid inferior brow. (C) Primary horizontal closure hidden along the inferior brow margin.

Figure 43-37. (A) BCC of the left lateral brow. (B) A 2.1 × 1.4 cm defect of the left lateral brow and upper lid. Note the degree of upper lid hooding representing an available tissue reservoir. (C) Arciform linear primary closure demonstrating appropriate laxity for closure and maintenance of brow shape.
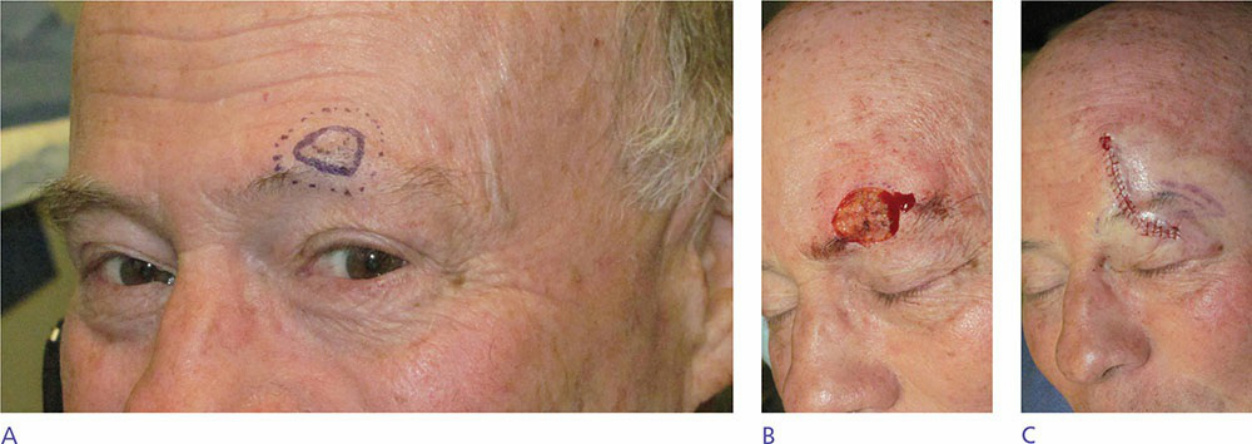
Figure 43-38. (A) MIS of the left mid-brow. (B) A 2.0 × 1.6 cm defect of the left mid-brow. (C) Vertically oriented closure of mid-brow defect. Note the brow marked for alignment and the arciform curvature designed across the orbital rim to minimize the net “pushing” effect of the vertical closure on the free lid margin.

Figure 43-39. (A) BCC of right medial brow. (B) A 1.1 × 0.9 cm defect of the right medial brow. (C) Vertically oriented primary closure, recapitulating the procerus rhytid/crease. Note the “pushing” effect at the inferior incision edge. (D) At 3-month postoperative result. Incision hides well in procerus crease and inferior tissue fullness/redundancy has dissipated.
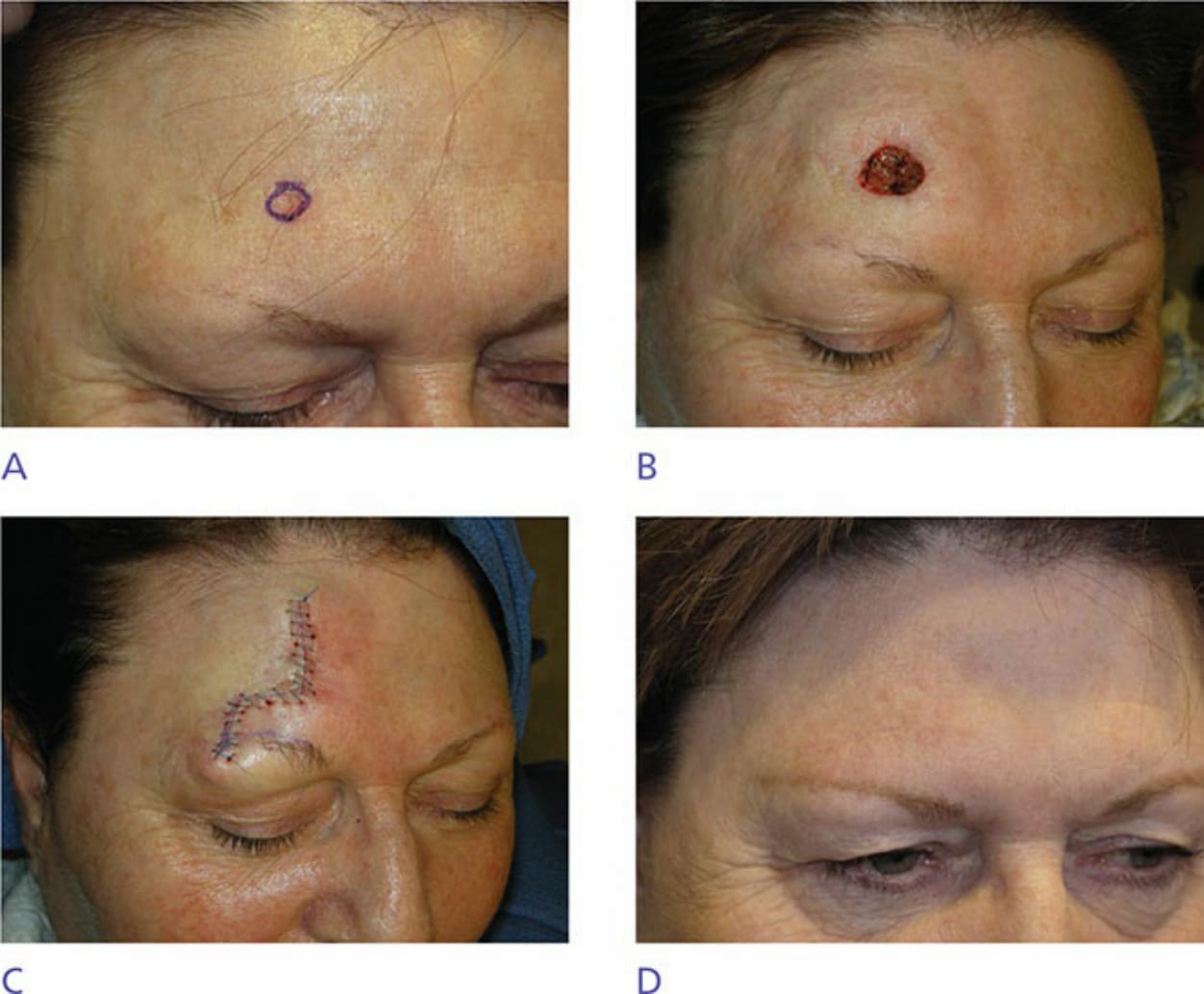
Figure 43-40. (A) BCC of the right mid-forehead. Note the sparse eyebrow hair present and absence of lateral brow. (B) A 1.4 × 1.2 cm defect of the right mid-forehead. Horizontal closure would result in brow elevation and vertical closure would result in removal of sparse brow hair. (C) Advancement flap sutured in place to hide incision along the frontal bossing ridge and displace the standing cone deformity laterally on the brow avoiding further loss of eyebrow hair. (D) At 3-month postop follow-up. Note symmetry of brow and salvage of medial brow hair.

Figure 43-41. (A) A 2.5 × 2.1 cm left suprabrow defect in a 46-year-old female patient with minimal tissue laxity/rhytides. (B) Burow’s advancement flap sutured in place. Careful attention to brow positioning must be given during flap design. (C, D). At 3-month postop result. Good maintenance of brow positioning and symmetry.

Figure 43-42. (A) MIS of the left medial suprabrow. (B) A 4.2 × 3.4 cm defect of the left medial/mid suprabrow. (C) Advancement flap sutured in place with laterally displaced Burow’s triangle. (D) At 3-month postop result. Good preservation of brow positioning and symmetry due to lateral displacement of standing cone deformity to the “crow’s feet” rhytides.

Figure 43-43. (A) BCC of the right lateral brow in a 52-year-old woman with minimal rhytides/skin laxity. (B) A 1.1 × 1.0 cm defect of the lateral brow. (C) Design of V-to-Y advancement flap. (D) V-to-Y advancement flap sutured in place. Careful alignment assured by premarking brow margins prior to tissue advancement.
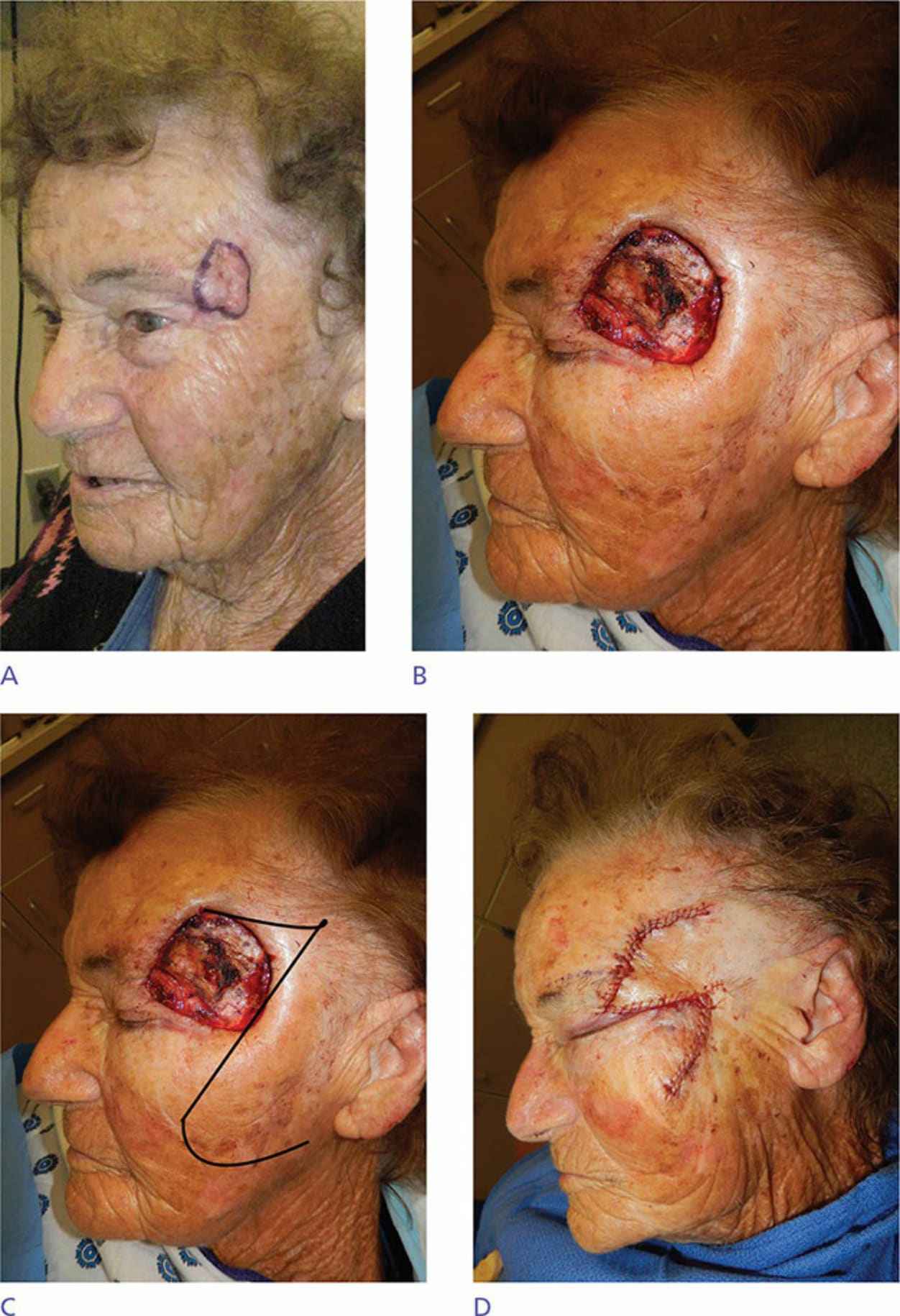
Figure 43-44. (A) Perineural SCC of the left lateral brow and temple. (B) A 6.3 × 6.0 cm defect through temporalis muscle involving the lateral brow, temple, and upper lid. (C) A rhombic transposition flap, incorporating laxity of the lateral cheek and preauricular skin, was planned. (D) Transposition flap from the lateral cheek/zygoma sutured in place.