ANATOMY
ANATOMY
An applied knowledge of local anatomy facilitates effective reconstruction of the forehead. This is a region supplied by a robust vasculature emanating from both the internal and external carotid artery systems. From medial to lateral, the main vessels include the dorsal nasal, supratrochlear, supraorbital, and the superficial temporal arteries. The supratrochlear and supraorbital arteries derive from the ophthalmic arterial branch of the internal carotid artery, and exit the skull through the supratrochlear and supraorbital foramen, respectively. These arteries ascend at approximately the level of the eyebrow, passing through the orbicularis and frontalis muscles and continuing superiorly in the superficial subcutaneous tissue.4 Extensive anastomoses ensure a robust supply to the forehead vasculature even when one or both of the supratrochlear and supraorbital branches are compromised.5 Laterally, the superficial temporal artery, the terminal branch of the external carotid artery, supplies the temple, lateral forehead, and eyebrow, in addition to the scalp. This vessel originates within the substance of the parotid gland and ascends to cross the zygoma anterior to the tragus. The superficial temporal artery becomes invested in the superficial temporal fascia above the zygomatic arch and subsequently gives off the parietal and frontal (anterior) branches (Fig. 43-4). The frontal branch of the superficial temporal artery runs just beneath the subcutis in the superficial fascia and is easily visualized intraoperatively. It is located just superficial and parallel to the temporal branch of the facial nerve, and thus serves as a rough landmark delimiting the depth to which undermining can safely be performed in this region.2
The sensory nerves of the forehead region derive from all three major branches of the trigeminal nerve. Medially, the supraorbital and supratrochlear nerves derive from the ophthalmic branch (V1). These nerves exit the cranium and quickly penetrate the musculature, running just above frontalis until they reach the mid-forehead, where they ascend to a more superficial subcuticular level. Surgical transection of the main nerve branches may result in transient or permanent anesthesia and/or significant
postoperative pain and lingering neuralgia. As such, horizontal closures should be undermined above the frontalis when possible, particularly on the lower forehead. More laterally, the zygomaticotemporal nerve, derived from the maxillary branch (V2) of the temporal nerve, exits its foramen and pierces the temporal fascia approximately 2.5 cm above the zygomatic arch. This small nerve helps innervate the lateral forehead and temple, where it communicates with the auriculotemporal branch of the mandibular nerve (V3). This latter nerve innervates the upper ear and lateral temple, ascending just anterior to the auricle. Accidental transection of the auriculotemporal nerve may lead to lingering numbness or neuralgia.2
The temporal branch of the facial nerve is responsible for motor innervation of the frontalis muscle. This nerve is susceptible to injury during procedures involving the temple and lateral eyebrow, and thus demands particular attention intraoperatively. Cadaveric dissection has demonstrated that temporal nerve ascends within the innominate fascia just deep to the SMAS over the zygoma, then continues slightly more superficially deep to the superficial temporal fascia.6 Upon reaching the frontalis, it courses along the undersurface of the musculature, with smaller branches penetrating superficially. Incisions and undermining anywhere from the zygomatic arch to the lateral eyebrow must remain superficial to the fascia to ensure the nerve is not damaged (Figs. 43-5 and 43-6).
The mimetic muscles of the forehead include the frontalis, procerus, corrugator supercilii, and the superior portion of the orbicularis oculi. These muscles intercalate with the overlying dermis through fibrous septae spanning the subcutis, thus animating the face. The frontalis is a large, flat muscle traversing the entire forehead. It originates at the superior aspect of the scalp, where its vertically oriented fibers insert directly into the galea aponeurotica, and extends inferiorly to interdigitate with the procerus, orbicularis oculi, and corrugators. Contraction of the frontalis elevates the eyebrows and induces the cutaneous horizontal creases defining RSTLs in this region. The twin corrugator muscles originate from the medial orbital rim just superior to the nose, and insert into the frontalis along with the dermis of the overlying eyebrows. Contraction in conjunction with the procerus muscle pulls the brows medially and inferiorly. The orbicularis oculi is located beneath the eyebrow, deep to the corrugator, and assists in closure of the eye.
There are essentially two potential undermining planes on the forehead, defined by their relationship to the mimetic musculature. A relatively avascular plane exists deep to the frontalis, just above pericranium. Although easily accessible and bloodless, the amount of laxity achieved even with wide undermining in this subgaleal plane is limited. Moreover, horizontally oriented incisions to this depth may damage
neurovascular structures. In contrast, undermining in the plane just superficial to the frontalis avoids the transection of larger vessels and sensory nerve bundles while concomitantly permitting substantial flap motion. Surgical technique in this plane must be meticulous, however, to maintain the relatively vulnerable overlying vasculature. Ultimately, the selection of the most appropriate undermining plane is informed by the size and location of the wound in relationship to neurovascular structures and reservoirs of native tissue laxity.
The anatomy of the temple is unique, with important implications in reconstructive surgery. Just beneath what is typically a thin layer of subcutaneous tissue is the temporoparietal fascia, a highly pliable 2–4 mm thick layer of richly vascularized connective tissue that envelops and protects branches of the temporal artery and the temporal branch of the facial nerve. In general, undermining should be performed just superficial to this fascial layer in order to preserve its associated neurovascular structures. Deep to the temporoparietal fascia is a fat pad with associated loose areolar tissue, which provides a relatively avascular plane for deeper resections and for raising a temporoparietal fascial flap (Fig. 43-7).7 Deeper still lies the temporalis fascia, the tough fibrous layer covering the temporalis muscle. Superiorly, the temporalis fascia consists of a single layer and attaches to the superior temporal line. Inferiorly, it divides into two layers that insert on the medial and lateral aspects of the zygomatic arch. The temporalis fascia is relatively strong and immobile, and thus may be useful for securing suspension sutures supporting a flap advanced from below. Finally, the temporalis muscle is just beneath the temporalis fascia. The temporalis is a broad, fan-shaped muscle of mastication that arises from the temporal fossa and passes deep to the zygomatic arch, where it inserts onto the coronoid process of the mandible.
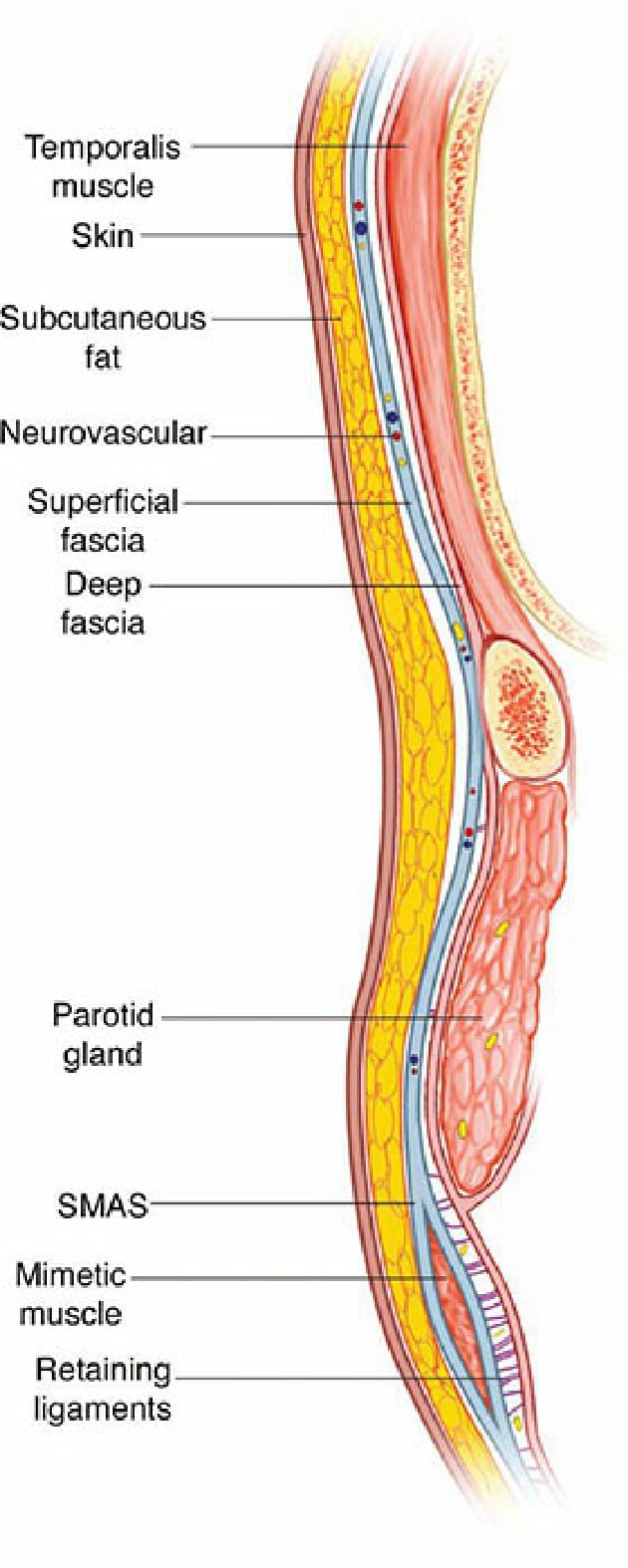
Figure 43-4. Layers of the forehead, coronal view. (By permission of Mayo Foundation for Medical Education and Research. All rights reserved).

Figure 43-5. Undermining above the temporoparietal fascia ensures the temporal branch of the facial nerve is not injured.
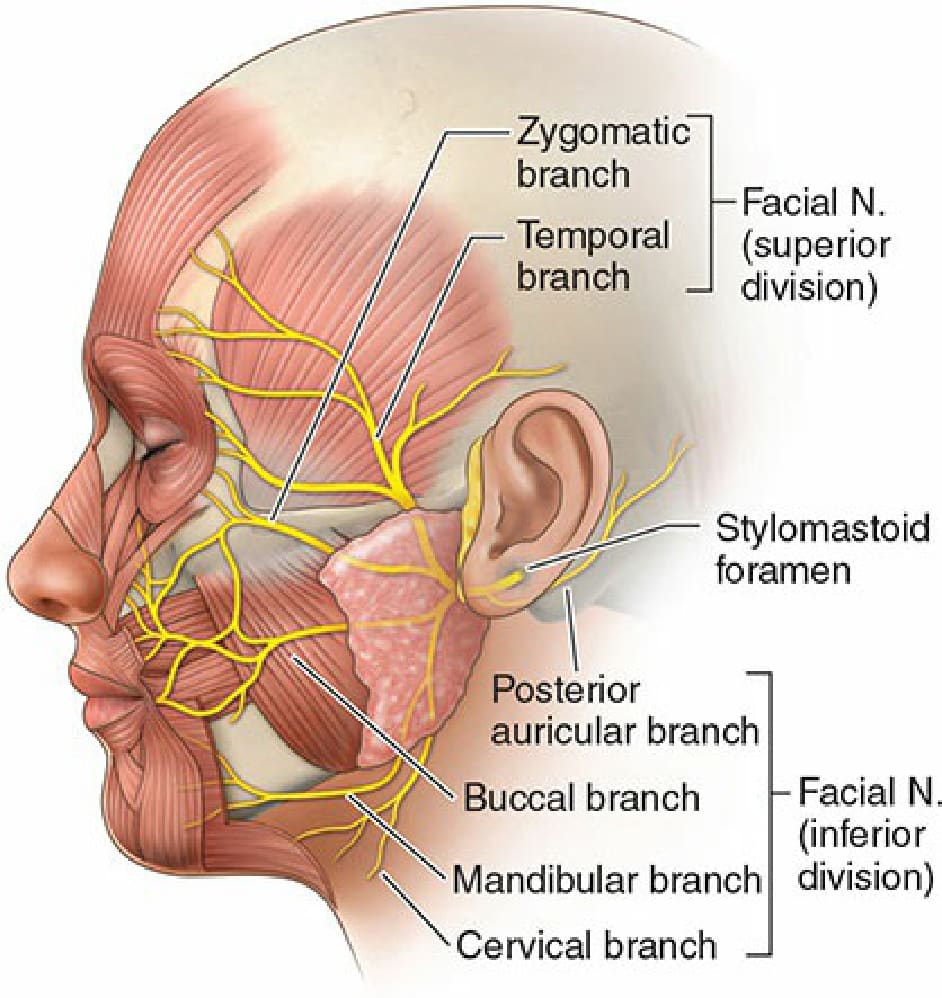
Figure 43-6. The course of the facial nerve.
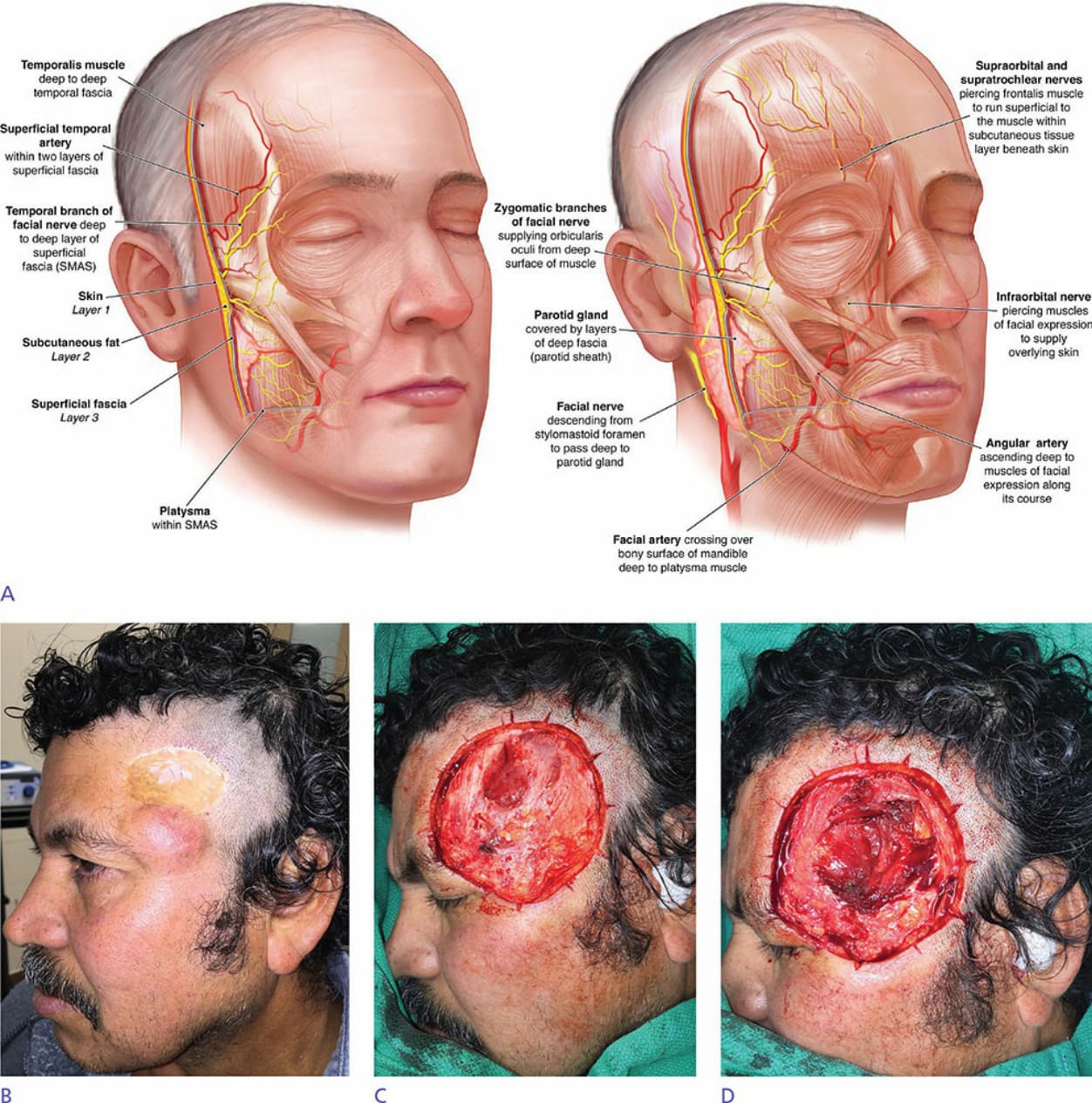
Figure 43-7. (A) Conceptual illustration demonstrating relationship of structures within layers of the face from superficial to deep. (B) This patient presented for Mohs extirpation of a recurrent dermatofibrosarcoma protuberans, which required removal of the tumor bulk inferiorly along with the adjacent split-thickness skin graft. (C) Preoperative MRI indicated the tumor did not penetrate the temporalis muscle, so the first stage was taken at the level of deep temporal fascia, except where the prior graft scar adhered to muscle superiorly. (D) Microinvasive disease was noted to penetrate the deep temporal fascia on frozen sections. A deeper layer including a superficial portion of temporalis muscle was required to clear the tumor, exposing the pericranial origin of the temporalis anteriorly, the muscle itself centrally, and the deep temporal fat pad inferiorly. (By permission of Mayo Foundation for Medical Education and Research. All rights reserved).